

Abstract
Objectives: Our primary objective was to examine the clinical presentation and explore differences between migrant and native individuals with first-episode psychosis at baseline. A secondary objective was to explore specific factors contributing to the observed clinical manifestations in first-generation migrant individuals with first-episode psychosis, such as childhood adversities, sex, age, and age at migration.
Methods: A naturalistic, observational, prospective, and case-control study was conducted. Statistical analyses included chi-squared tests for categorical variables, t-tests for continuous variables, ANOVA tests for comparisons between multiple groups, and multivariate generalized linear models to explore factors associated with clinical presentation in first-generation migrants. Results were considered statistically significant at p < 0.05.
Results: Out of the sample of 363 subjects, 114 were first-generation migrants and 249 were native-born patients. In terms of clinical presentation, first-generation migrants had significantly higher scores on the PANSS Negative subscale compared to natives (p < 0.01). Further analysis showed that this difference was driven by higher average scores in first-generation migrants compared to non-migrants (p < 0.027). First-generation migrants exhibited higher levels of childhood adversity compared to non-migrants. Multivariate analysis revealed that sex was a significant predictor of PANSS Negative scores in first-generation migrants, with men having higher scores than women.
Conclusion: In our study, first-generation migrants, particularly men, showed more severe negative symptoms compared to natives. These findings support that the migratory condition should be considered when assessing subjects with first-episode psychosis, as this will help to characterise the pathology precisely and provide personalized clinical treatments.Resumen
Objetivos: El primer objetivo fue examinar la presentación clínica y analizar las diferencias entre migrantes y nativos en la visita basal. El segundo objetivo fue explorar factores específicos que pudieran contribuir en la presentación clínica de los migrantes de primera generación con primeros episodios psicóticos, como las adversidades infantiles, el sexo, la edad y la edad de migración.
Métodos: Se llevó a cabo un estudio naturalista, observacional, prospectivo, de casos y controles. Los análisis estadísticos incluyeron pruebas de chi-cuadrado para variables categóricas, pruebas de T-Student para variables continuas, pruebas de ANOVA para comparaciones entre múltiples grupos y un modelo lineal generalizado para explorar los factores asociados con la presentación clínica en migrantes de primera generación. Los resultados se consideraron estadísticamente significativos con p < 0.05.
Resultados: De la muestra de 363 sujetos, 114 eran migrantes de primera generación y 249 eran nativos. Los migrantes de primera generación obtuvieron puntuaciones significativamente más altas en la subescala Negativa del PANSS en comparación con los nativos (p < 0.01). Un análisis adicional mostró que esta diferencia se debía a puntajes promedio más altos en migrantes de primera generación en comparación con no migrantes (p < 0.027). Los migrantes de primera generación reportaron niveles más altos de adversidad infantil en comparación con los no migrantes. El análisis multivariado reveló que el sexo sería un predictor significativo de los puntajes negativos del PANSS en migrantes de primera generación, teniendo los hombres puntajes más altos que las mujeres.
Conclusiones: Los migrantes de primera generación, particularmente los hombres, presentaron mayor severidad de síntomas negativos en comparación con los nativos. Estos hallazgos respaldan la importancia de considerar el estatus migratorio al evaluar a los sujetos con primeros episodios psicóticos, ya que esto ayudará a una caracterización más precisa de la patología y la implementación de tratamientos clínicos personalizados.Palabras clave: Migración; Presentación clínica; Primeros episodios Psicóticos; Síntomas negativos.
Keywords: Migration; Clinical presentation; First-episode psychosis; Negative symptoms.
INTRODUCTION
Migration has become a global phenomenon involving 281 million migrants, 3.60% of the world’s population in 2020 (1). In the community of Madrid, INE statistics revealed that 14% of the population in 2022 were immigrants. With the increasing number of migrant individuals, the need to understand its implications, particularly on the development of mayor mental health conditions such as psychosis, has become apparent.
Psychosis refers to a wide range of psychological symptoms that lead to a loss of contact with reality. It is estimated that between 1.5 and 3.5 per cent of the world population will meet the diagnostic criteria for a psychotic disorder in their lifetime (2). There is consistent evidence that stress related to major life events such as migration is a risk factor for psychosis (3,4). A recent meta-analysis revealed that first- and second- generation migrants from outside Europe have a higher risk (3-6%) of developing psychosis compared to Europeans (1-2%)(5). The underlying causes of the increased risk for psychosis between migrants have been explored in previous studies. Proposed explanatory hypotheses include the intertwin of a number of epidemiological, psychological, biological and social factors (3,6,7). A multinational European study has shown that social disadvantages and adversities during the migration experience are associated with an increased risk of psychosis in first-generation migrants (8). In addition, traumatic experiences are also a risk factor for psychosis, and migrants have been found to report a greater exposure to cumulative trauma (7) than general population.
In terms of clinical presentation, studies have also explored the influence of ethnicity and migration. Concerning ethnic differences, a Cambridge study found evidence that individuals of Black and North African ethnicity experienced more positive symptoms than those of White ethnicity (9).Consistent with this, a study conducted in the Netherlands revealed that first- and second-generation immigrants from Morocco exhibited higher symptom scores, on both positive and negative symptoms, compared to native Dutch individuals (10). However, findings are heterogeneous. A recent Canadian study found no difference in the prevalence of positive and negative symptoms between migrants and non-migrants (11). This is similar to some previous studies, that found no differences in clinical scales between groups (12,13).
Moreover, in addition to identifying migrants’ risk of developing psychosis, it is important to assess their outcomes and how they differ from non-migrants. Symptomatic outcomes for people who develop first-episode psychosis (FEP) are highly variable, about half of individuals achieve complete remission of symptoms and no further episodes, while others have a more persistent, refractory course (14). Several factors have been associated with the course of FEP, some of these include cannabis use, biological, social and ethnic factors (15). It is thus reasonable to assume that some of these and other related factors, may be expressed differently in migrants. For instance, according to a recent systematic review, immigrants with first-episode psychosis are more likely to achieve remission and often have higher rates of involuntary admission (16). It is acknowledged that clinical management and prognosis of psychosis is influenced by clinical presentation. Therefore, exploring whether migration experience influences clinical presentation may contribute to a greater understanding and improvement of the experience lived by these minority groups.
We hypothesised that migration experience would have an impact on the clinical expression at the time of presentation in first episode psychosis (FEP), resulting in greater severity of symptoms in migrants. Consequently, the primary aim of the current study was to examine the clinical presentation and to explore the differences between migrant and non-migrant individuals with FEP at baseline. A secondary objective was to explore specific factors that might be contributing to the observed clinical manifestations in the subgroup of migrant individuals with FEP, that has been previously associated to clinical presentation or migration status such as the presence of childhood adversities, sex, age, and the age at migration.
METHODS
a. Study design
This is a naturalistic, observational, prospective, case-control first episode of psychosis study. Data was gathered from a regional consortia for the study of “Environment and Genes interaction in Schizophrenia – Community of Madrid research group (AGES-CM)”, a multicentric study that involves seven University Hospitals in Madrid, Spain (i.e. La Paz University General Hospital, Gregorio Marañón University General Hospital, 12 de Octubre University General Hospital, La Princesa University Hospital, Ramón y Cajal University Hospital, San Carlos University General Hospital and Fundación Jimenez Díaz). Recruitment started in 2014 and it is still ongoing. Subjects admitted for a first- episode psychosis, first degree relatives and matched controls were recruited in each of the participating hospitals and associated community centres. Only first-episode participants recruited from 2013 to 2023 were included for this study purpose. The study was approved by the correspondent ethical committees at each clinical centre. Methods were designed and assessments were conducted according to the Declaration of Helsinki principles, international and national guidelines. All participants and/or their legal guardians gave written informed consent before participation.
b. Participants
From February 2013 to July 2023, 417 participants with FEP were recruited for the AGES-CM study. A total of 363 subjects out of this sample had completed the variables of interest (e.g. migrant status, sex, ethnicity, PANSS Negative) and were thus selected for the current study. FEP participants were selected according to the following inclusion and exclusion criteria. The inclusion criteria were: 1) age between 7 and 40 years at the time of the baseline initial assessment; 2) persistence of positive psychotic symptoms for less than 24 months in the context of a FEP according to DSM-IV criteria. Individuals with the following criteria were excluded: 1) concurrent diagnosis of another Axis I mental disorder, other than substance abuse or dependence; 2) intellectual disability if functioning was impaired before the onset of the disorder; 3) history of neurodevelopmental disorder or traumatic head injury with loss of consciousness; 4) pregnancy.
c. Sociodemographic and migrant status
Sociodemographic data including age, sex, ethnicity, and socioeconomic status was collected at the baseline clinical interview (i.e. study entrance). Ethnicity was divided into 3 groups for descriptive purposes only: Caucasic, Hispanic and Others. The parental socioeconomic status (SES) was evaluated using the Hollingshead’s Index of Social Position (17). The scale is comprised of five levels (Class I = highest level, Class V = lowest level), reflecting both occupational status and educational achievement. The original SES was re-coded into one categorical variable with 3 groups: low (classes V and IV), middle (class III) and high (classes II and I). For migration status, personal migration was considered, subdividing the sample into two groups (yes=first generation migrants, no=natives). In addition, based on parental migration experience, they were divided into 3 groups (1st generation migrants, 2nd generation migrants and non-migrants). First-generation migrants (1st G migrants) were defined as individuals born in a foreign country. Second-generation migrants (2nd G migrants) were identified as individuals born in Spain with at least one parent who was a first-generation migrant. Individuals not complying with those definitions were considered as non-migrants.
d. Clinical assessment
Clinical evaluation was performed by trained psychiatrists in the use of the correspondent clinical instruments with inter-rater reliability of at least 80% using the interclass correlation coefficient. The Positive and Negative Syndrome Scale (PANSS) (18) was used to assess the severity of symptoms in a 7 point Likert-scale; ranking levels of psychopathology in increasing order from 1= “absent” to 7= “extreme”. The Positive, Negative, and General Psychopathology dimensions were computed, then the total score was calculated for each of the subscales. The PANSS scale demonstrated highly satisfactory internal consistency in our sample, with Cronbach’s alpha coefficients for each dimension as follows: 0.81 for the Positive Scale, 0.86 for the Negative Scale, and 0.85 for the General Scale.
To assess the severity of depression, The Hamilton Depression Rating Scale (19) was used. It contains 21 items, rated on a 3- or 5-point Likert-scale. Total score was computed. The internal consistency, measured by Cronbach’s alpha, was 0.82 for the total scale.
The Young Mania Rating Scale (20) was used to assess the severity of manic symptoms. It is based on 11 items rated on a 5-point Likert-scale. A total score was calculated. In our sample the scale’s internal consistency was α = 0.76.
e. Childhood adversity and bullying
Childhood adversity that occurred before the age of 17 was collected using an adapted version of the Childhood Experience of Care and Abuse Questionnaire (CECA.Q)(21). Participants completed a retrospective self-report questionnaire. The current study focused on nine forms of childhood adversity: (i) physical abuse inflicted by one or both parental figures; (ii) sexual abuse perpetrated by a person ≥ 5 years older; (iii) death of one or both biological parents; (iv) emotional abuse by parental figures; (v) neglect; (vi) separation from one or both parent-figures for ≥ 6 months; (vii) household poverty, (viii) parental discord; (ix) expelled or suspended from school and/or high-school. Each item was dichotomised using the most conservative published cut-off points (21). A “total adversity” variable (range 0-9) was calculated with the dichotomised item scores. It was recoded on a categorical variable of 0 (none), 1 (one or two adverse experiences), 2 (multiple adverse experiences).
For bullying, the participants were asked if they had experienced any type of bullying before the age of 17 (having been verbally abused or made fun of; having been ignored, excluded, or left out on purpose; having been hit, kicked, shoved, or locked in a room; or any other type of bullying). For the analyses, a categorical variable with three groups 0 (never), 1 (occasionally), 2 (frequently) was recoded.
f. Statistical analyses
Analyses were performed using SPSS v25.0. Data normality distribution was explored using Kolmogorov-Smirnov test. Continuous variables are described by mean, median, and standard deviation. Chi-squared tests x2 frequency analyses were employed to describe the differences in categorical variables and T-tests were used to test differences in continuous variables for descriptive analyses.
First, exploratory analyses were made to examine the differences in clinical presentation (i.e. severity of symptoms) between first generation migrants and those considered as “natives” (non-migrants and 2nd generation migrants) using T-test.
Further analyses explored the differences between the 3 migration groups (non-migrants, 1st generation migrants and 2nd generation migrants), using analyses of variance ANOVA tests. Levene’s test was conducted to assess the homogeneity of variances, guiding the selection of the correspondent post-hoc tests. Post-hoc analyses were then used to identify differences between specific groups, with the Games-Howel test being used for non-homogeneous variances and the Scheffe test for homogeneous variances. A non-parametric Kruskal-Wallis test was used to analyse the differences between categorical variables in the three groups.
Secondary analyses were conducted in the first-generation migration FEP group only, in order to further explore the plausible influence of other factors that had previously been associated with migration status (such as the presence of childhood adversities, sex, age and the age at migration) on clinical presentation in this group. A Multiple General Lineal Model (GLM) was conducted to explore the variables that might influence the presence of significant differences in symptom presentation at baseline among first-generation migrants. Predictive variables (i.e. sex, childhood adversities, age, age at migration) were selected according to the literature on the clinical presentation and migration status of first-episode psychosis (22,23,24,25). For all analyses, p values < 0.05 were used to indicate statistical significance.
RESULTS
a. Sample characteristics
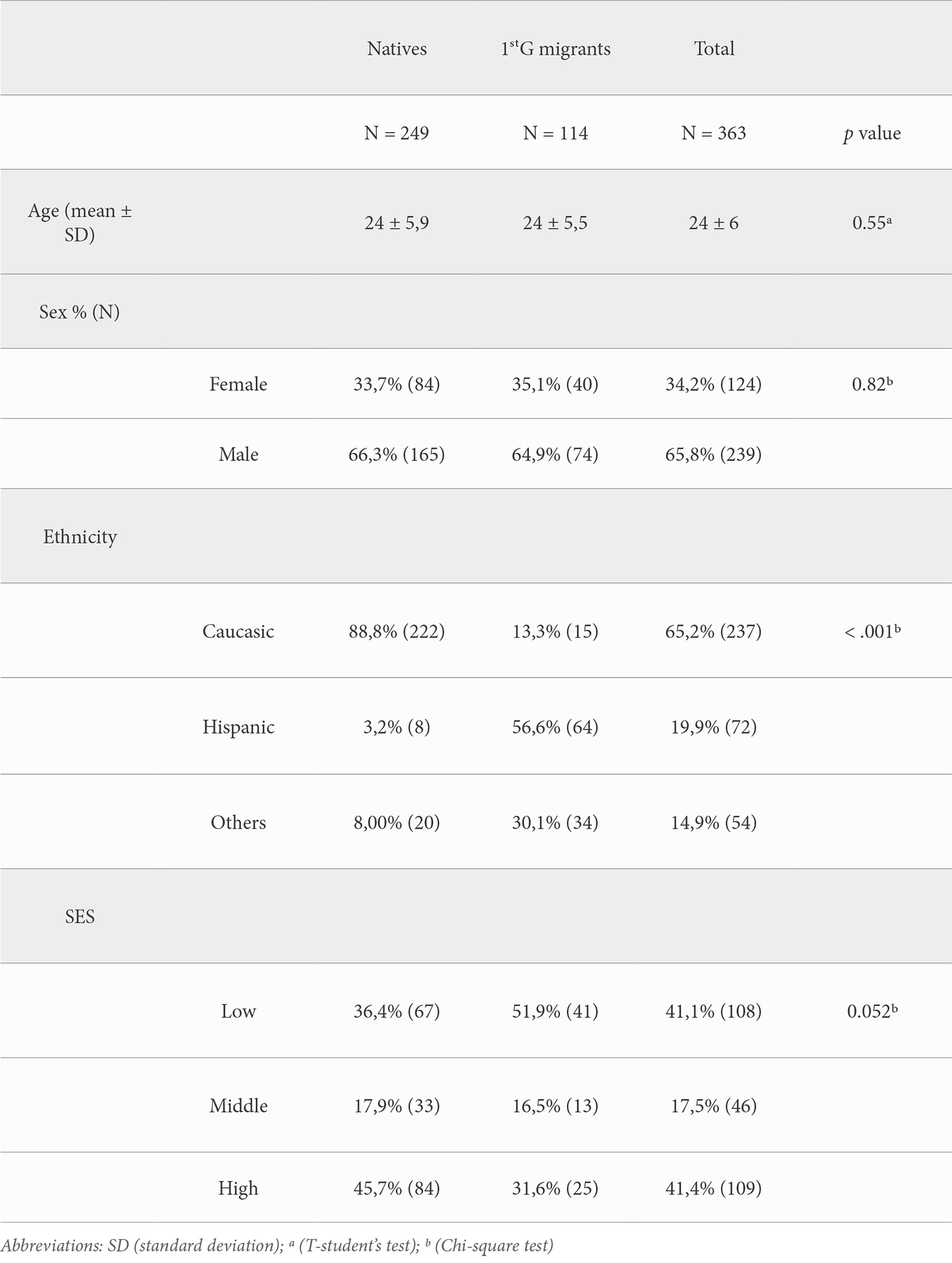
Out of the sample of 363 subjects, there were 114 who were 1st generation migrants (34,2%) and 249 native-born patients (non-migrants and 2nd generation migrants) (65,95%). No significant differences were found in age, sex, and SES. Significant differences (p < 0,001) were found between “natives” and 1st generation migrants in terms of ethnicity. The socio-demographic characteristics are presented in Table 1.
b. Clinical presentation
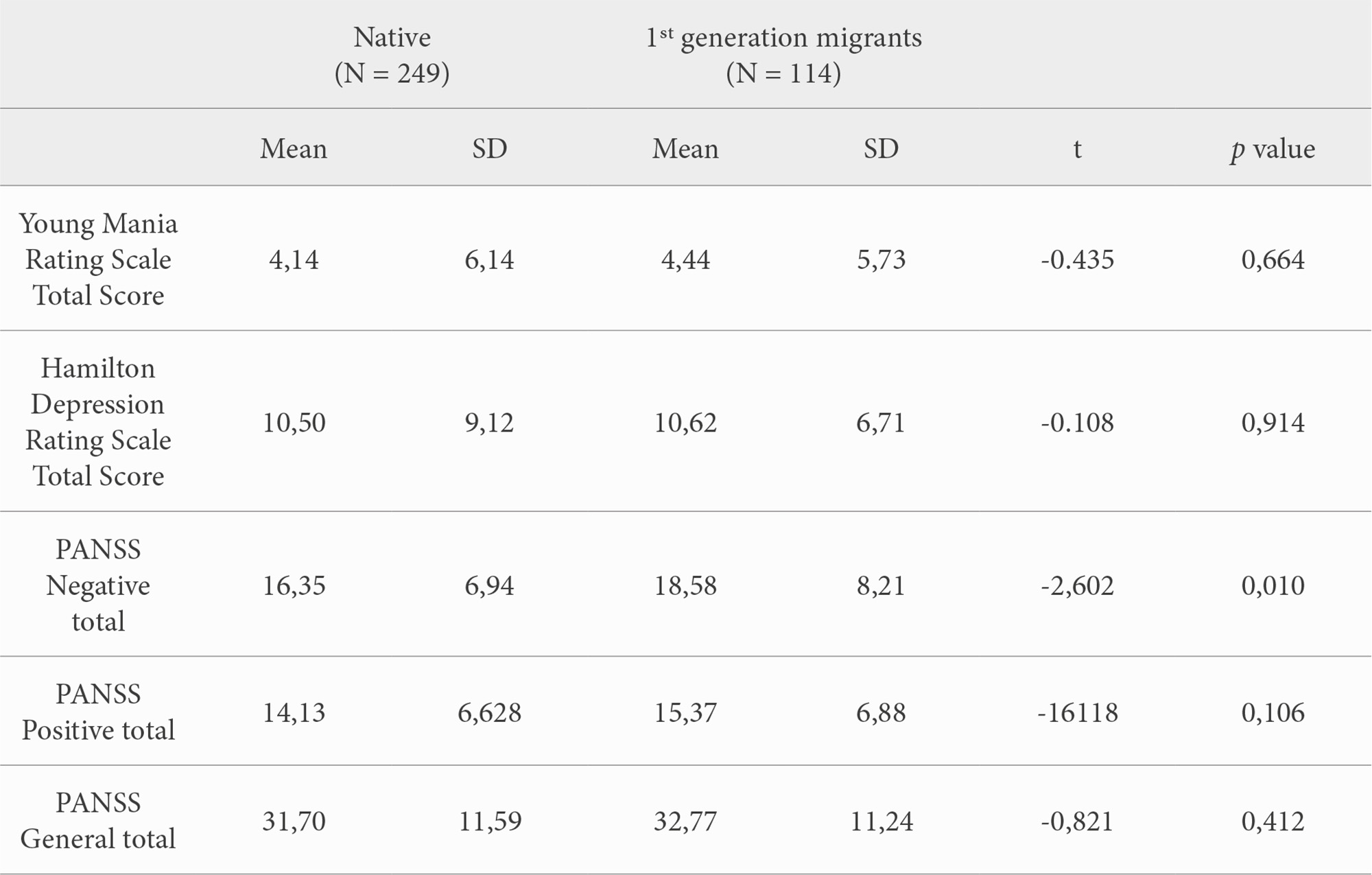
On the clinical scales, a significant difference (p < 0.01) was found for negative symptom presentation, assessed using the total of the PANSS Negative subscale, between migrants and natives; with 1st generation migrants scoring 2 points higher on average than natives. No other significant differences were found. All the t-tests performed on the correspondent clinical scales are listed in Table 2.
Further analyses were made to explore the differences between the 3 groups (1st Generation migrants, 2nd Generation migrants and non-migrants). ANOVA analyses replicated a significant difference (p < 0,027) for the PANSS Negative Total between groups. Post-hoc analysis demonstrated the significant difference in the severity of negative symptom presentation was derived by higher average scores in 1st generation migrants vs. non-migrants, with the first-generation migrant group having more severe (i.e. two points higher) negative symptoms than the later non-migrant group.
c. Childhood adversities and bullying
Kruskal-Wallis test revealed a significant difference in childhood adversity scores across the 3 groups (non-migrants, 1st G migrants and 2nd G migrants) (x2= 8.767, p < .012). Post-hoc comparisons demonstrated that the median of childhood adversity for the 1st Generation migrants (Md = 2) was significantly (p < .011) higher than the median for the non-migrant group (Md = 1). No significant difference was found for bullying scores between the 3 groups.
d. Other plausible factors related to clinical presentation or migration
The Multivariate Generalized Linear Model (GLM) including sex, childhood adversities, age and age at migration was not statistically significant (R2= 0.029, F(5,95) = 1.607, p = 0.166) for the PANSS negative in the first-generation migration group. However, it was found that sex alone significantly predicted PANSS Negative in 1st generation migrants (B = -3.592, p = 0.041). For instance, in the 1st generation migrant group, women were estimated to have a mean score of -3.592 points lower on the PANSS Negative than men in our migrant FEP group. The remaining variables (i.e childhood adversities, age, and age at migration) did not exhibit a significant effect on the PANSS Negative scale in this group.
DISCUSSION
In this study, we investigated the impact of migration on the clinical presentation of first-episode psychosis. Additionally, we explored some of the variables that might contribute to the symptomatology in FEP first-generation migrant individuals. Our results revealed more severe negative symptoms in first-generation migrants than in non-migrants at the baseline clinical interview. First generation migrants were found to report higher levels of childhood adversity than non-migrants. According to our findings, sex emerges as a predictive factor for negative symptoms among first-generation migrants, with men having higher scores.
Several studies have previously demonstrated that migration experience influences the clinical characteristics of psychosis (3). Congruent with this notion, our results highlight the difference in negative symptoms severity between migrants and non-migrants at the time of presentation of the FEP. However, these results are not aligned with those of previous studies that showed more severity of positive symptoms at first contact in first-generation migrant groups (8), or no differences in any clinical scale between migrants and non-migrants (13). Nevertheless, the assessment of negative symptoms is complex and requires a specific training. Therefore, the hostile environment faced by first-generation migrants and the ethnic variability may lead the examiner to interpret greater negative symptomatology on them compared to non-migrants (26).
Consistent with previous literature, we found a greater cumulative exposure to childhood adversity in first-generation migrants with FEP (25). These findings have been previously linked to an increased risk of psychosis in this group (27). Regarding its plausible impact on clinical presentation, negative symptoms were not associated with total childhood adversities as assessed in our study. This might be congruent with previous research suggesting that childhood adversities are associated with greater severity of hallucinations and delusions (28).
With regards to sex, previous studies found men to experience more negative symptoms than women, regardless of migrant status (24). Our results were as expected, they support that these sex differences in clinical presentation are preserved among migrants. Sex-specific stressors of migration have been explored in previous literature. Prior research suggests that men experience more migration-related stress and discrimination (29). This, combined with traditional gender roles in which men are expected to be strong and in control, may make it more difficult for men to seek help (30). All this can lead to a greater severity in the clinical presentation at diagnosis, with greater negative symptoms.
Strengths and limitations
To the best of our knowledge, this is the first and largest comparative study between migrants and non-migrants with FEP in Spain regarding their clinical presentation at the time of admission in our clinical services. Our study was derived form a large representative multi-centre sample in the autonomous community of Madrid. It includes different ethnic groups beyond the North-African, which had been the most studied migration group in our country to date. All relevant information was collected using validated instruments and standardised data entry to minimise collection bias across sites.
However, there are several limitations in this study. First, the total sample for the main study cohort comprised 417 participants, however our analyses were conducted on a smaller sample (N=363) due to incomplete data at baseline. Although the sample size is smaller than the original recruitment, it remains sufficiently large to ensure adequate statistical power for producing reliable results. Second, the presence of childhood adversities were rated using a retrospective self-report questionnaire, and therefore the results should be approached with caution (31). The choice of instrument is justified since reports of childhood adversity obtained retrospectively from people with psychotic disorders are stable over time (32). Additionally, it has been qualitatively reclassified into 3 groups, leading to a loss of information. Our recoding was made based on previous articles (33). Finally, there are factors that may affect clinical presentation that were not considered in the study, such as substance use, family psychiatric history or duration of untreated psychosis. It would be interesting to further explore other factors, such as those mentioned above, that may influence the clinical presentation of psychosis in migrants and to gain a more complete picture.
CONCLUSION
The migration experience has an impact on the clinical presentation of first psychotic episodes in first-generation migrants. In our study, first-generation migrants, particularly migrant men, experienced more negative symptoms than natives (i.e. non migrants or second-generation migrants) at baseline. In line with the above, the migratory condition may be considered when assessing subjects with FEP, as this will help to characterise the pathology precisely and provide personalized clinical treatments.
CONFLICT OF INTEREST STATEMENT
Dr. Arango has been a consultant to or has received honoraria or grants from Abbot, Acadia, Ambrosetti, Angelini, Biogen, Boehringer, Gedeon Richter, Janssen Cilag, Lundbeck, Medscape, Menarini, Minerva, Otsuka, Pfizer, Roche, Sage, Servier, Shire, Schering Plough, Sumitomo Dainippon Pharma, Sunovion, Takeda and Teva.
Dr Arango has received support by the Spanish Ministry of Science and Innovation, Instituto de Salud Carlos III (ISCIII), co-financed by the European Union, ERDF Funds from the European Commission, “A way of making Europe”, financed by the European Union – NextGenerationEU (PMP21/00051), PI19/01024. PI22/01824 CIBERSAM, Madrid Regional Government (B2017/BMD-3740 AGES-CM-2), European Union Structural Funds, European Union Seventh Framework Program, European Union H2020 Program under the Innovative Medicines Initiative 2 Joint Undertaking: Project PRISM-2 (Grant agreement No.101034377), Project AIMS-2-TRIALS (Grant agreement No 777394), Horizon Europe, the National Institute of Mental Health of the National Institutes of Health under Award Number 1U01MH124639-01 (Project ProNET) and Award Number 5P50MH115846-03 (project FEP-CAUSAL), Fundación Familia Alonso, and Fundación Alicia Koplowitz.
REFERENCES
- ↑Interactive World Migration Report 2022 [Internet]. [citado 1 de abril de 2024]. Disponible en: https://www.iom.int/wmr/interactive
- ↑Calabrese J, Al Khalili Y. Psychosis. En: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [citado 8 de abril de 2024]. Disponible en: http://www.ncbi.nlm.nih.gov/books/NBK546579/
- ↑Morgan C, Knowles G, Hutchinson G. Migration, ethnicity and psychoses: Evidence, models and future directions. World Psychiatry. 2019; 18(3): 247-258.
- ↑Selten JP, Ven E van der, Termorshuizen F. Migration and psychosis: a meta-analysis of incidence studies. Psychol Med. 2020; 50(2): 303-313.
- ↑Dealberto MJ. Why are immigrants at increased risk for psychosis? Vitamin D insufficiency, epigenetic mechanisms, or both? Med Hypotheses. 2007; 68(2): 259-267.
- ↑Tarricone I, D’Andrea G, Jongsma HE et al. Migration history and risk of psychosis: Results from the multinational EU-GEI study. Psychol Med. 2022; 52(14): 2972-2984.
- ↑Quattrone D, Di Forti M, Gayer-Anderson C et al. Transdiagnostic dimensions of psychopathology at first episode psychosis: Findings from the multinational EU-GEI study. Psychol Med. 2019; 49(8): 1378-1391.
- ↑Veling W, Selten JP, Mackenbach JP, Hoek HW. Symptoms at first contact for psychotic disorder: Comparison between native Dutch and ethnic minorities. Schizophr Res. 2007; 95(1): 30-38.
- ↑Anderson KK, Rodrigues R. Differences in clinical presentation at first hospitalization and the impact on involuntary admissions among first-generation migrant groups with non-affective psychotic disorders. Soc Psychiatry Psychiatr Epidemiol. 2023; 58(9): 1329-1341.
- ↑Stouten LH, Veling W, Laan W, Van der Gaag M. Psychopathology, cognition and outcome in Dutch and immigrant first-episode psychosis patients. Early Interv Psychia. 2019; 13(3): 646-656.
- ↑Comparing the clinical presentation of first-episode psychosis across different migrant and ethnic minority groups in Montreal, Quebec [Internet]. [citado 7 de abril de 2024]. Disponible en: https://journals.sagepub.com/doi/epdf/10.1177/070674371205700505
- ↑Lally J, Ajnakina O, Stubbs B et al. Remission and recovery from first-episode psychosis in adults: Systematic review and meta-analysis of long-term outcome studies. Br J Psychiatry. 2017; 211(6): 350-358.
- ↑Murray RM, Mondelli V, Stilo SA et al. The influence of risk factors on the onset and outcome of psychosis: What we learned from the GAP study. Schizophr Res. 2020; 225: 63-68.
- ↑Maguire J, Sizer H, Mifsud N, O’Donoghue B. Outcomes for migrants with a first episode of psychosis: a systematic review. Schizophr Res. 2020; 222: 42-48.
- ↑Hollingshead AB. Four factor index of social status. Yale J Sociology. 2011; 8: 21-51.
- ↑Kay SR, Fiszbein A, Opler LA. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophrenia Bull. 1987; 13(2): 261-276.
- ↑Hamilton M. A rating scale for depression. J Neurol, Neurosur Ps. 1960; 23: 56-62. [Internet]. [citado 28 de marzo de 2024]. Disponible en: https://jnnp.bmj.com/content/23/1/56
- ↑Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: Reliability, validity and sensitivity. Brit J Psychiat. 1978; 133(5): 429-435.
- ↑Bifulco A, Bernazzani O, Moran PM, Jacobs C. The childhood experience of care and abuse questionnaire (CECA.Q): Validation in a community series. Brit J Clin Psychol. 2005; 44(4): 563-581.
- ↑Pablo GS de, Catalan A, Serrano JV et al. Negative symptoms in children and adolescents with early-onset psychosis and at clinical high-risk for psychosis: Systematic review and meta-analysis. Brit J Psychiat. 2023; 223(1): 282-294.
- ↑Burns JK, Jhazbhay K, Esterhuizen T, Emsley R. Exposure to trauma and the clinical presentation of first-episode psychosis in South Africa. J Psychiat Res. 2011; 45(2):179-184.
- ↑Carter B, Wootten J, Archie S, Terry AL, Anderson KK. Sex and gender differences in symptoms of early psychosis: a systematic review and meta-analysis. Arch Womens Ment Health. 2022; 25(4): 679-691.
- ↑D’Andrea G, Lal J, Tosato S et al. Child maltreatment, migration and risk of first-episode psychosis: Results from the multinational EU-GEI study. Psychol Med. 2023; 53(13): 6150-6160.
- ↑Vega WA, Lewis-Fernández R. Ethnicity and variability of psychotic symptoms. Curr Psychiatry Rep. 2008; 10(3): 223-228.
- ↑Varchmin L, Montag C, Treusch Y, Kaminski J, Heinz A. Traumatic events, social adversity and discrimination as risk factors for psychosis – An Umbrella Review. Front Psychiatry. 2021; 12: 665957. doi: 10.3389/fpsyt.2021.665957.
- ↑Bailey T, Álvarez-Jiménez M, García-Sánchez AM, Hulbert C, Barlow E, Bendall S. Childhood trauma is associated with severity of hallucinations and delusions in psychotic disorders: a systematic review and meta-analysis. Schizophrenia Bull. 2018; 44(5): 1111-1122.
- ↑Assari S, Lankarani MM. Discrimination and psychological distress: Gender differences among Arab Americans. Front Psychiatry. 2017; 8:23. doi: 10.3389/fpsyt.2017.00023. PMID: 28265246; PMCID: PMC5316930.
- ↑Smith GD, Hebdon M. Mental health help-seeking behaviour in men. J Adv Nurs. 2024; 80(3): 851-853.
- ↑Pinto RJ, Maia ÂC. A comparison study between official records and self-reports of childhood adversity. Child Abuse Rev. 2013; 22(5): 354-366.
- ↑Fisher HL, Craig TK, Fearon P et al. Reliability and comparability of psychosis patients’ retrospective reports of childhood abuse. Schizophr Bull. 2011; 37(3): 546-553.
- ↑Ajnakina O, Trotta A, Forti MD et al. Different types of childhood adversity and 5-year outcomes in a longitudinal cohort of first-episode psychosis patients. Psychiatry Res. 2018; 269: 199-206.
Celso Arango López
Real Academia Nacional de Medicina de España
C/ Arrieta, 12 · 28013 Madrid
Tlf.: +34 91 547 03 18 | E-Mail: secretaria@ranm.es
Año 2024 · número 141 (02): 126-133
Enviado: 25.03.24
Revisado: 01.04.24
Aceptado: 07.05.24