

Abstract
Postabortion ovarian vein septic thrombophlebitis is a very rare variety with high complication rates and it should be considered as a differential diagnosis for febrile abdominal pain syndrome in the post-abortion period. The contrast-enhanced CT or MRI have the highest sensitivity and specificity to diagnose the ovarian veins thrombi. The treatment it consists in a combination of anticoagulation therapy and antibiotics. In case that anticoagulation is contraindicated it´s recommended placing an inferior vena cava filter.
Resumen
La tromboflebitis de las venas ováricas es una variedad muy rara con altas tasas de complicaciones y que se debe plantear como diagnóstico diferencial ante un síndrome de dolor abdominal febril en el periodo posterior al aborto. La TC o RM con contraste intravenoso tienen la mayor sensibilidad y especificidad para diagnosticar los trombos de las venas ováricas. El tratamiento consiste en una combinación de terapia anticoagulante y antibióticos. En caso de que la anticoagulación esté contraindicada se recomienda colocar un filtro de vena cava inferior.
Keywords: Ovarian veins; Postabortion; Ovarian veins thrombophlebitis; Postabortion ovarian vein thrombosis.
Palabras clave: Venas ováricas; Postaborto; Tromboflebitis; Tromboflebitis de las venas ováricas; Trombosis de las venas ováricas postaborto.
INTRODUCTION
Postabortion ovarian vein septic thrombophlebitis is a cause of pathological puerperium, being an uncommon but serious condition (1,2). It is associated with certain risk factors such as emergency cesarean section, prolonged labor, premature rupture of membranes, chorioamnionitis, pelvic inflammatory disease, secondary to gynecological surgery or malignant factors. Pathophysiologically the thrombosis is explained due to intimal damage of the pelvic veins caused by the spread of uterine infection, the pro-coagulant state of pregnancy and pelvic venous ectasia (3). All of this will predispose to the formation of septic thrombi (3). The right ovarian vein will be affected in 90% of the cases, since the retrograde venous reflux in the left ovarian vein during delivery protects it from bacterial dissemination (3). The clinical scenario usually presents between the second to fifth day after delivery, with nonspecific symptoms (vomiting, nauseas, right or left lower quadrant abdominal pain, sepsis) and persistent fever that does not yield with antibiotics (1,2).
CLINICAL CASE
36-year-old woman hospitalized for late abortion (24 weeks of gestation) and chorioamnionitis, treated with antibiotics. She has a worsening left-sided lower abdominal pain. Physically, pelvic tenderness without peritonism or urinary complaints. Laboratory tests consistent with severe inflammatory state including leukocytosis (17.000 cells/mmc) and elevated C-reactive protein (326 mg/L). After 48 hours of treatment, she persists with fever and worsening of her general condition. An abdominal ultrasound is performed without significant findings. Given the bad evolution of the patient a CT is requested.
IMAGING FINDINGS
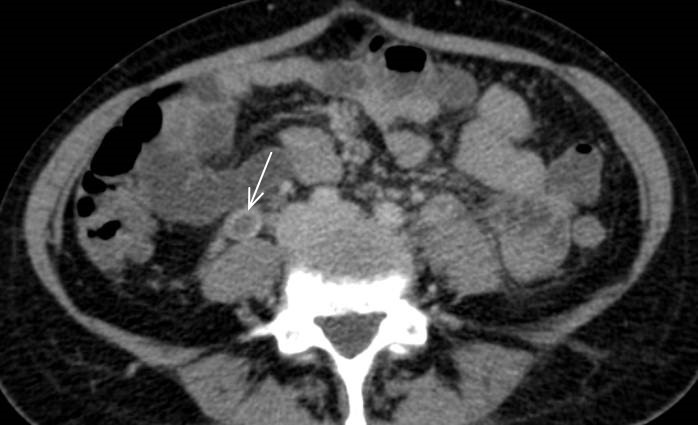
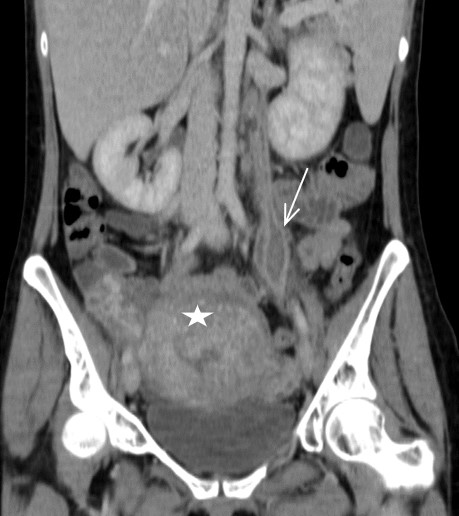
In the contrast enhanced CT (portal venous phase), a postpartum uterus is observed, with the presence of hypodense material occupying and distending both ovarian veins (Fig.1a-1b) from the uterus up to the renal vein on the left (Fig. 2a) and to the inferior vena cava to the right (Fig. 2b). There is associated thickening and enhancement of the walls of the ovarian and uterine veins. No free fluid, collections or lymphadenopathy were observed.


DISCUSSION
Ovarian vein thrombophlebitis is a difficult diagnosis, so there must be a high clinical suspicion and the final diagnosis will be reached through imaging studies. Usually, ultrasonography with Doppler examination is the first technique performed since is less expensive and requires no contrast material (3). Contrast-enhanced CT and MRI have the highest sensitivity and specificity to diagnose the ovarian veins thrombi (4). Normally, the CT examination shows a tubular retroperitoneal mass with a central low attenuation extending from the ovaries to the renal vein on the left or to the inferior vena cava on the right.
The differential diagnosis is made mainly with appendicitis, tubo-ovarian abscess and renal colic. CT is highly sensitive for these diseases. In appendicitis we can identify a structure that arise from the cecum inferior to the ileo-cecal junction and on CT it can be associated with fat stranding near the vermiform structure and also with hyperdense foci within the lumen. Tubo-ovarian abscess is the late complications of pelvic inflammatory disease and on CT we can find a tubular configuration fluid attenuation pelvic masses which may show a thick enhancing wall and may contain fluid-fluid levels or gas. Renal colic is a pattern of abdominal pain most commonly caused by ureteric calculi. The pain is felt in the loin radiating down to the groin because of the peristalsis or spasm of the ureter. The calculi it can be easily identified on CT.
MR imaging is appropriate in the diagnosis and follow-up of the ovarian vein thrombophlebitis. MR have better depicts tissue contrast without IV contrast material comparing with CT. The MR due to its sensitivity to blood flow and to the paramagnetic effects of iron can differentiate flowing blood, acute thrombus and subacute thrombus (4).
The treatment for the ovarian vein thrombophlebitis will consist in a combination of anticoagulation therapy for a duration of 3-6 months and antibiotics (5). If not treated about 50% of patients will present septic pulmonary embolisms or other complications like acute obstruction of a ureter, ovarian infarction (3). In case that anticoagulation is contraindicated, because of the high risk of spreading the thrombosis it´s recommended placing an inferior vein cava filter(6).
Given the early diagnosis of our patient, she received timely treatment, with clinical improvement and resolution of the thrombi in a follow-up CT performed 3 months later.
REFERENCES
- Bilgin M, Sevket O, Yildiz S, Sharifov R, Kocakoc E. Imaging of postpartum ovarian vein thrombosis. Case Rep Obstet Gynecol. 2012;2012:134603.
- Dessole S, Capobianco G, Arru A, Demurtas P, Ambrosini G. Postpartum ovarian vein thrombosis: an unpredictable event: two case reports and review of the literature. Arch Gynecol Obstet. 2003;267(4):242-246.
- Virmani V, Kaza R, Sadaf A, Fasih N, Fraser-Hill M. Ultrasound, computed tomography, and magnetic resonance imaging of ovarian vein thrombosis in obstetrical and nonobstetrical patients. Can Assoc Radiol J. 2012;63(2):109-118.
- Bannow BTS, Skeith L. Diagnosis and management of postpartum ovarian vein thrombosis. Hematol Am Soc Hematol Educ Progr. 2017; 2017(1):168-171.
- Kominiarek MA, Hibbard JU. Postpartum ovarian vein thrombosis: an update. Obstet Gynecol Surv. 2006;61(5):337-342.
- Lenz CJ, Wysokinski WE, Henkin S, Cohoon KP, Casanegra A, Simmons BS, et al. Ovarian Vein Thrombosis. Obstet Gynecol. 2017;130(5):1127-1135.
CONFLICT OF INTEREST STATEMENT
The authors of this article declare that they have no conflict of interest with respect to what is expressed in this work.
Anca Oprisan
Servicio de Radiología. Área Clínica de Imagen Médica
Hospital Universitario y Politécnico La Fe. Valencia
C/ Pere Bonfill, 5, 3º piso, puerta 5 · 46008 Valencia
Tlf.: +34 91 159 47 34 | E-Mail: oprisan.anca@gmail.com
An RANM. 2021;138(02): 180 – 182
Enviado: 30.06.21
Revisado: 16.07.21
Aceptado: 28.07.21