

Abstract
Objective: To determine and analyze the prevalence of the principal risk factors in patients with penile cancer in General Hospital “Dr. Eduardo Liceaga” and their survival rate at 24 months.
Methods: Cross-sectional, descriptive study. The population (n=93) are hispanic, adult male residents of Mexico City with penile cancer diagnosed. The variables analyzed are: Age, smoking status, HPV status, presence of vascular invasion, treatment and survival status after 24 months.
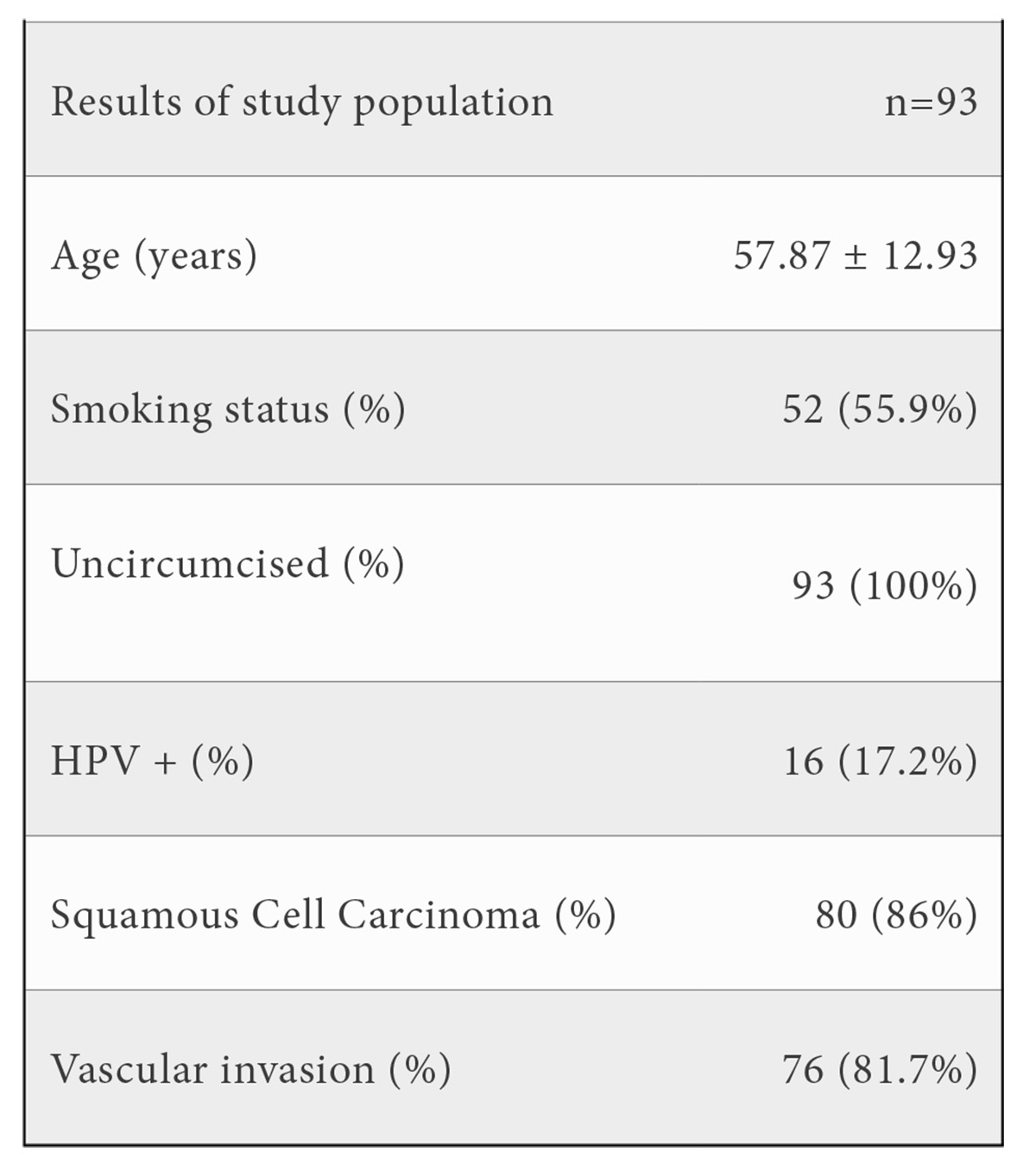
Results: Mean age (n=93) was 57.87. 55.9% were active smokers. 100% were uncircumcised. Only 17.2% were HPV +. Squamous Cell Carcinoma was the predominant type with 86%. 18.3% had vascular invasion. At 24 months after diagnosis with treatment 84.9% patients were alive, 6.5% died of cancer related causes, 6.5% of other causes and (2.2%) of chemotherapy toxicity.
Conclusion: This infrequent disease requires a high quality multidisciplinary treatment. Squamous cell carcinomas are the predominant type in Mexico City, risk factors such as smoking, uncircumcised, age and HPV infection were present. HPV vaccines in men could help reduce a proportion of malignancies but there is no data related. Adjuvant therapy should be considered since the survival rate at 24 months of study was lower than first world countries. Periodic evaluation of chemotherapy adverse effects should be considered since a significant proportion died because of toxicity.Resumen
Introducción: El cáncer de pene es una neoplasia rara. Tiene una incidencia de 0,91 por 100.000 varones. La mayoría de los carcinomas son de origen escamoso. La incidencia varía según la circuncisión, prácticas de higiene, fimosis, infección por VPH y exposición al tabaco.
Objetivo: Determinar y analizar la prevalencia de los principales factores de riesgo en pacientes con cáncer de pene en el Hospital General “Dr. Eduardo Liceaga” y su tasa de supervivencia a los 24 meses.
Métodos: Estudio transversal, descriptivo. La población (n=93) son hombres adultos hispanos residentes de la Ciudad de México con diagnóstico de cáncer de pene. Las variables analizadas son: edad, tabaquismo, VPH, invasión vascular, tratamiento y supervivencia a los 24 meses.
Resultados: La edad media (n=93) fue de 57,87 años. El 55,9% eran fumadores activos. El 100% no estaban circuncidados. Solo el 17,2% eran VPH+. El Carcinoma de Células Escamosas fue el tipo predominante con un 86%. El 18,3% tuvo invasión vascular. A los 24 meses del diagnóstico con tratamiento el 84,9% de los pacientes estaban vivos, el 6,5% fallecieron por causas relacionadas con el cáncer, el 6,5% por otras causas y (2,2%) por toxicidad de quimioterapia.
Conclusión: Enfermedad poco frecuente, requiere tratamiento multidisciplinario de alta calidad. Los carcinomas de células escamosas son el tipo predominante en la Ciudad de México, se presentaron factores de riesgo como tabaquismo, no circuncidado, edad e infección por VPH. Las vacunas contra el VPH en hombres podrían ayudar a reducir una proporción de tumores malignos, pero no hay datos relacionados. Se debe considerar la terapia adyuvante ya que la tasa de supervivencia a los 24 meses de estudio fue menor que en países del primer mundo. Se debe considerar la evaluación periódica de los efectos adversos de la quimioterapia ya que una proporción significativa murió debido a la toxicidad.Keywords: Squamous cell carcinoma; Chemotherapy; Circumcision; Mortality rate for penile cancer; Oncourology; Hispanic population.
Palabras clave: Carcinoma de células escamosas; Quimioterapia; Circuncisión; Tasa de mortalidad por cáncer de pene; Oncourología; Población hispana.
INTRODUCTION
Penile cancer has an incidence of 1/100,000 males, becoming a rare malignancy in the world. (1) Developing countries have a higher incidence than non-developing ones, having 6% of all malignant neoplasms. (2) Mexico has an incidence rate of 0.91 per 100,000 males and 0.31% of the total malignant neoplasms, resulting in a mortality rate of 0.2 per 100,000, representing 0.17% of cancer deaths (3,4).Most male patients with penile cancer are older, with a mean age on the sixth decade. The diagnosis is between 50-70 years old (5,6). Most penile carcinomas are of squamous (SCC) origin (95%). (2). The incidence diverges according to some practices, such as phimosis, sexual partners, HPV infection, circumcision practice, tobacco exposure, and other factors (7,8). Cigarette smokers have 3 to 4.5 times fold-risk of developing penile cancer (9,10). Recently, penile invasive SCC and its variants, as well as precursor lesions, are divided into two major categories: related and non-related to HPV (11).
Basaloid, warty, and warty basaloid carcinomas are included in the HPV-related group, while typical, verrucous, papillary, sarcomatoid, pseudohyperplastic, and cuniculatum carcinomas are included in the other category. Small to intermediate basophilic, undifferentiated, or basaloid cells make up the majority of HPV-related cancers, whereas highly keratinized, differentiated squamous cells make up the majority of HPV-negative tumors (11,12,13) Penile carcinoma typically starts as a tiny lesion that spreads throughout the entire glans, shaft, and corpora. The lesion can be papillary and exophytic or flat and ulcerative, and if left untreated, it can lead to penile auto-amputation. Although the development rates of papillary and ulcerative lesions are similar, the flat, ulcerative tumor has a higher risk of nodal metastasis and has a 5-year survival rate. (14) Although most lesions are limited to either the foreskin or the glans, a subset of cases shows the involvement of multiple compartments, in some cases extending into the glans, coronal sulcus, and foreskin’s inner mucosa. Multifocal lesions are found in approximately 15% of cases (15).
Before starting any treatment, a microscopic analysis of a biopsy specimen is required to confirm the diagnosis of penile cancer, as well as to determine the degree of invasion, the existence of vascular invasion, and the histologic grade of the lesion. (16) Penile preservation techniques have been more popular in recent years as it has become clear that this sort of surgery for a primary cancer is linked to improved functional outcomes and psychological well-being (17). Penile cancer involving the redundant preputial and penile skin can be adequately treated with circumcision. Because glansectomy can be used to treat penile cancer involving the spongy erectile tissue of the glans, excision can save the corpora cavernosa, and reconstruction is confined to a redefinition or covering surgery of the distal corporal bodies. Often, just grafting the tips of the corporal bodies provides an excellent function as well as cosmetic result (18). Minimally invasive treatments such as imiquimod or 5-fluorouracil (5-FU) topical chemotherapy, laser therapy, or brachytherapy can be used to treat precancerous alterations or early-stage malignancies (19,20). Patients with untreated inguinal metastases rarely live longer than two years. After surgical care, patients with stage I or II malignancies that are still restricted to the penis at the time of diagnosis had a 5-year survival rate of roughly 85%. The 5-year survival rate for stage III and IV malignancies is roughly 59%. The 5-year survival rate for cancer that has spread to other regions of the body is 11% (16). Circumcision, male vaccination of HPV, early treatment of phimosis, smoking cessation, and hygiene practices are some of the potential techniques for preventing penile cancer. Some of these measures would necessitate a thorough cost-benefit analysis as well as significant changes in global health policy (21). Because of the disease’s rarity, data collection and standardization in clinical practice have been limited.
MATERIAL AND METHODS
This is a descriptive cross-sectional study. The participants in the research (n=93) are hispanic, adult male patients and residents of Mexico City Metropolitan area with penile cancer diagnosed by a pathology report of Mexico General Hospital “Dr. Eduardo Liceaga”, a tertiary care hospital in Mexico City. The inclusion criteria considered for this study were: male adults between 20-90 years at the date of diagnosis, diagnosis of penile cancer with a pathological report and treated in Mexico General Hospital “Eduardo Liceaga” between 2013-2019 with a 24 month follow-up. Exclusion criteria was loss of follow up, pathological report of other dysplastic diseases of the penis and age. 168 medical files were examined and 75 were excluded because of loss of follow up or pathology report inconsistent with penile cancer. The variables of interest analyzed in this study are: Age, smoking status, HPV status, pathology report of biopsied specimen, presence of vascular invasion, curative treatment used, and survival status at 24 months after diagnosis.
RESULTS
The mean age of the group of study (n=93) was 57.87 (SD ± 12.93). 52 (55.9%) were active smokers and 41 (44.1%) never smoked. 93 (100%) were uncircumcised. 77 (82.1%) patients were HPV (-) by pathology report and 16 (17.2%) were HPV (+). Squamous Cell Carcinoma (SCC) was the predominant type of cancer in our group with 80 (86%) of the cases with a pathology report of SCC and 13 (14%) reported as other variants of penis carcinoma. 76 (81.7%) patients did not have vascular invasion and 17 (18.3%) had vascular invasion.
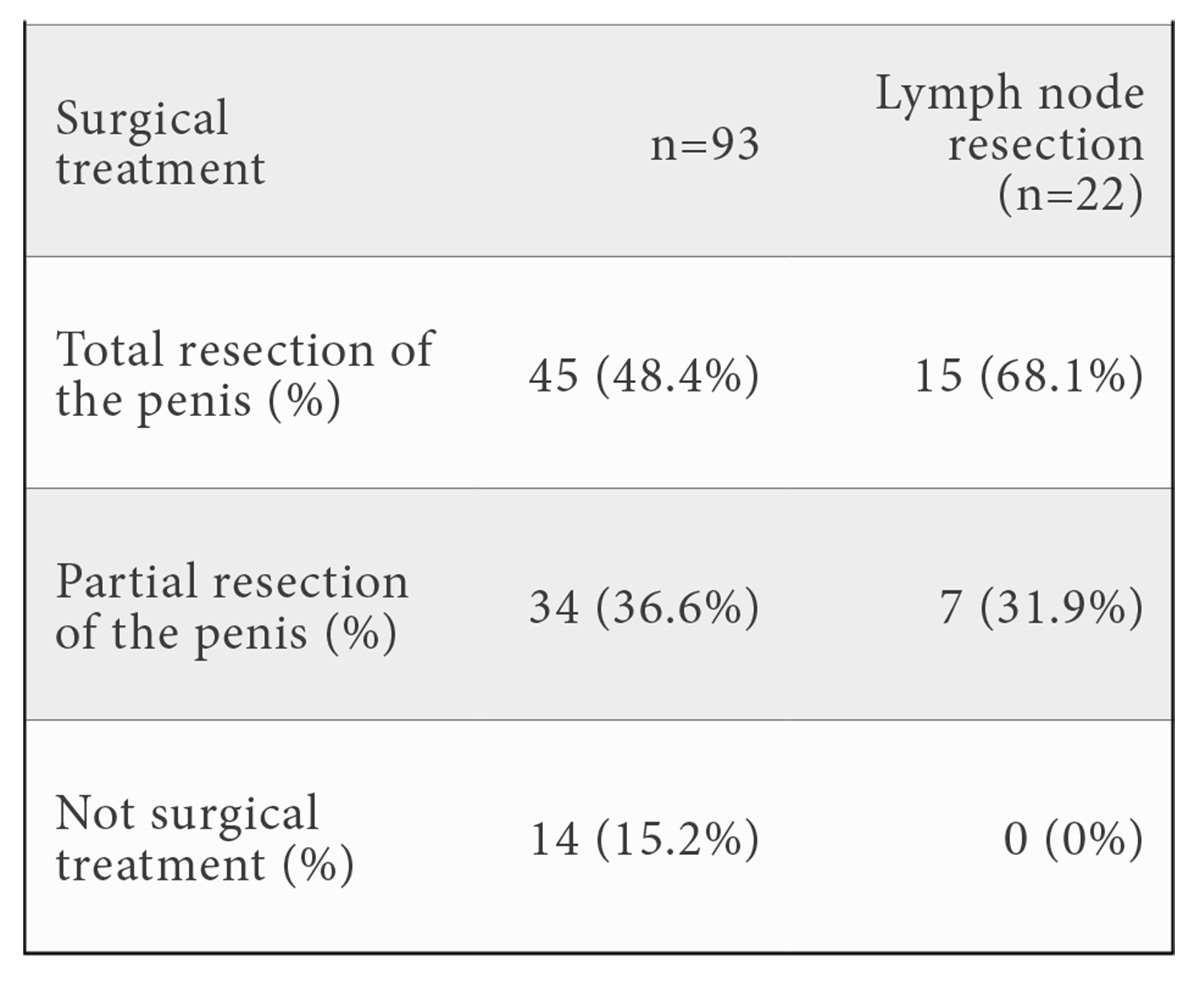
The treatment for penis cancer in the study group included surgical total resection, surgical partial resection, adjuvant chemotherapy and adjuvant radiotherapy. 45 (48.4%) had total resection of the penis, 34 (36.6%) had partial resection of the penis and 14 (15.1%) of the patients did not have surgical management. 21 (22.5%) had lymph node resection.
81 (87.1%) patients did not require adjuvant chemotherapy and 12 (12.9%) were treated with adjuvant chemotherapy and radiotherapy.

At 24 months after diagnosis 79 (84.9%) patients were alive, 6 (6.5%) died of cancer related causes, 6(6.5%) died of other causes and 2 (2.2%) died of chemotherapy toxicity.

DISCUSSION
The results of the study show the prevalence of the principal risk factors for penile cancer mentioned previously in literature (9,10,11) and the frequency that these are present in a tertiary care hospital. The mean age at diagnosis was at the sixth decade of life (57 years), the same reported in the Mexican population previously by Chaux et al. (5,6) while in the United States the mean age of presentation is at 70 years (24). More than half of the population of our study group were smokers (55.9%), smoking is known to be a risk factor for penile squamous cell carcinoma and multiple malignancies (25). All of the patients of the study were uncircumcised, in Mexico the circumcision prevalence ranges between 10-31% and this could be attributed to the fact that circumcision is a protective factor for penile cancer and a higher incidence in countries with low circumcision prevalence (24,25) such as Mexico. Pathology results indicated that 86% of the penile malignancies were squamous cell carcinoma (non-HPV-related) and 14% reported as other malignancies (HPV-related-malignancy). Immunohistochemical analysis reported 82.1% of the specimens to be HPV negative and this could correlate with the percentage of SCC (86% of non-HPV-related malignancy) reported in the group of study, while 17.2% were HPV positive (14% of HPV-related-malignancy). 18.3% had vascular invasion and all of these patients had surgical treatment. 84.9% of patients had surgical treatment and the rest were candidates for laser ablation (26). The majority of the patients did not require adjuvant chemotherapy (87.1%), In patients with locally progressed or cN2–3 disease, professional opinion supports the use of neoadjuvant combination chemotherapy with cisplatin and a taxane (27), or adjuvant radiotherapy (87.1 percent), which is only advised for tumors less than 4cm and T1 and T2.
Survival rate at 24 months was 84.9%. 6 deaths were cancer related and 5 of these cancer related deaths were not treated with adjuvant chemotherapy nor adjuvant radiotherapy. Sentinel node biopsy in a centralized care system has been shown to reduce 5-year mortality rates by 7% in the UK and 9% in the Netherlands. (23), this approach should be implemented in a way to increase survival rates and do further research. Centralization of penile cancer treatment also demonstrated that it improves survival rate when referring patients to high-volume centers through correct pathological reporting and treatment (28). Because topical medications can be used to treat premalignant illness, circumcision should be the first surgical choice (29). For superficial lesions, laser ablation therapy has been employed with good functional results (30). External beam irradiation and interstitial brachytherapy are two penis-preserving methods for limited situations. In penile cancer, lymph node metastases are common. All patients with lymph node metastases that have been confirmed histologically should have a radical bilateral inguinal lymphadenectomy. The mainstay of treatment for locally invasive PSCC is surgery.
The European Association of Urology’s current guidelines encourage using organ-sparing surgery wherever possible, in which the original tumor is entirely removed while leaving as much functional length and anatomical features of the penis as possible intact. In higher-risk individuals, larger tumors infiltrating the corpora cavernosa or surrounding organs necessitate disfiguring procedures such as partial or total penectomy (23).
CONCLUSIONS
Penile cancer is an infrequent disease that requires a high-quality multidisciplinary treatment in which the urologist and oncologist are the main pillar for the management. Squamous cell carcinomas are the predominant type of penile cancer, risk factors reported in literature such as smoking, uncircumcised penis, age and HPV infection were present in our population at different degrees. It is important to highlight the relevance of circumcision as a preventive method for penile cancer, besides the lower risk of infection of HPV, since Mexico has a low circumcision prevalence. HPV vaccines in men could help to reduce a proportion of penile malignancies but there is no data related that have become available. Because the study group’s survival rate at 24 months was lower than that of first-world nations, adjuvant therapy should be considered according to the most recent guidelines. Periodic evaluation of chemotherapy adverse effects, and serum concentration of the drug should be also considered since a significant proportion of the population died because of chemotherapy toxicity.
ACKNOWLEDGEMENTS
I want to thank to Dr. Rosas-Nava, Dr. Acevedo and all the Urology team of the Mexico General Hospital who were part of the care of each patient that provided valuable information for this article.
Special thanks to my wife Janeth Leon who helped me in the translation and correction of grammatical errors of this article. My daughter Isabel who is a great inspiration for all the things I do.
ETHICAL POLICY
This protocol complies with the requirements of the Declaration of Helsinki since care was taken to protect the health of the population in all aspects during the protocol.
No procedure was performed that should be considered harmful and unnecessary for the patient during the protocol, on the contrary, the improvement of their health status was always sought. The procedures carried out comply with the regulations of the General Health Law regarding health research, complying with the corresponding articles.
The project is submitted for evaluation by the Ethics Committee of the ABC Medical Center, for its approval, to be able to publish it later.
FUNDING
No funding was needed for this publication.
BIBLIOGRAPHY
- Djajadiningrat RS, Van Werkhoven E, Meinhardt W et al. Penile sparing surgery for penile cancer: does it affect survival? J Urol. 2014; 192(1): 120-125. https://doi.org/10.1016/j.juro.2013.12.038
- Vieira CB, Feitoza L, Pinho J et al. Profile of patients with penile cancer in the region with the highest worldwide incidence. Sci Rep. 2020; 10: 1-7.
- Jiménez Ríos MA, Solares Sánchez M, Martínez Cervera P et al. Penile cancer. INCAN Mexico. 2011. http://incan-mexico.org/revistainvestiga/elementos/documentosPortada/1298053577.pdf
- Reynoso N, Scavuzzo A, Santana Rios Z et al. Cáncer de pene en México: 20 años de experiencia en un hospital académico de tercer nivel (Penile cancer in Mexico: Twenty years experience at a tertiary academic hospital). Arch Esp Urol. 2020; 73(1):11-18. Spanish. PMID: 31950918.
- Chaux A, Velázquez EF, Amin A et al. Distribution and characterization of subtypes of penile intraepithelial neoplasia and their association with invasive carcinomas: a pathological study of 139 lesions in 121 patients. Hum Pathol. 2012; 43: 1020-1027.
- PDQ Adult Treatment Editorial Board. PDQ Cancer Information Summaries (Internet). National Cancer Institute (US); Bethesda (MD): 2021. Penile Cancer Treatment (PDQ®): Health Professional Version.
- Slongo J, Giuliano AR, Johnstone PA, Spiess PE. The relationship between HPV and penile cancer: Filling a knowledge gap in the general population. Can Urol Assoc J. 2019; 13(2): 38.
- Cubilla AL, Lloveras B, Alejo M et al. The basaloid cell is the best tissue marker for human papillomavirus in invasive penile squamous cell carcinoma: a study of 202 cases from Paraguay. Am J Surg Pathol. 2010; 34: 104-114.
- Daling JR, Madeleine MM, Johnson LG et al. Penile cancer: Importance of circumcision, human papillomavirus and smoking in in situ and invasive disease. Int J Cancer. 2005; 116(4): 606-616. doi: 10.1002/ijc.21009. PMID: 15825185.
- Tsen, HF, Morgenstern H, Mack T, Peters RK. Risk factors for penile cancer: Results of a population-based case-control study in Los Angeles County (United States). Tsen HF, Morgenstern H, Mack T, Peters RK. Risk factors for penile cancer: Results of a population-based case-control study in Los Angeles County (United States). Cancer Causes Control. 2001 Apr;12(3):267-77. 2001; 12(3): 267-277. http://www.jstor.org/stable/3553680.
- Cubilla AL, Lloveras B, Alejo M et. al.: The basaloid cell is the best tissue marker for human papillomavirus in invasive penile squamous cell carcinoma: a study of 202 cases from Paraguay. Am J Surg Pathol. 2010; 34(1): 104-114.
- Jayaraj R, Kumarasamy C, Sabarimurugan S, Madhav MR. Meta-analysis of penile cancer: Conceptual interpretations. Lancet Oncol. 2019; 20(3): e125-e125. https://doi.org/10.1016/S1470-2045(19)30023-3
- Slongo J, Giuliano AR, Johnstone PA, Spiess PE. The relationship between HPV and penile cancer: Filling a knowledge gap in the general population. Can Urol Assoc J. 2019; 13(2): 38.
- Partin AW, Dmochowski RR, Kavoussi LR, Peters CA, Wein AJ, editors. Campbell Walsh Wein Urology. Philadelphia: Elsevier, 2020.
- Cubilla AL, Dillner J, Amin MB et. al. Tumours of the penis: Malignant epithelial tumours. En: Moch H et al. World Health Organization classification of tumours: Pathology and genetics of tumours of the urinary system and male genital organs. Lyon: IARC, 2016. p. 262-276.
- Engelsgjerd JS, LaGrange CA. Penile cancer. (Updated 2021). En: StatPearls [Internet]. Treasure Island (FL): StatPearls; 2022. https://www.ncbi.nlm.nih.gov/books/NBK499930/
- Hegarty PK, Eardley I, Heidenreich A et al. Penile cancer: Organ‐sparing techniques. BJU Int. 2014; 114(6): 799-805. https://doi.org/10.1111/bju.12338
- Monstrey S, D’Arpa S, Claes K et al. Plastic surgery: Volume 4: Lower extremity, trunk, and burns, 2018; 13: 292-322.e3
- Hakenberg OW, Compérat EM, Minhas S, Necchi A, Protzel C, Watkin N. European Association of Urology: Penile cancer. Eur Urol. 2015; 67: 142-150. https://uroweb.org/guideline/penile-cancer/
- Zhu Y, Gu WJ, Xiao WJ et al. Important therapeutic considerations in t1b penile Cancer: Prognostic significance and adherence to treatment guidelines. Ann Surg Oncol. 2019; 26(2): 685-691.
- Minhas S, Manseck A, Watya S, Hegarty PK. Penile cancer: Prevention and premalignant conditions. Urology. 2010; 76(2): S24-S35. https://doi.org/10.1016/j.urology.2010.04.007
- Hakenberg OW, Dräger DL, Erbersdobler A, Naumann CM, Jünemann KP, Protzel C. The diagnosis and treatment of penile cancer. Dtsch Arztebl Int. 2018; 115(39): 646-652. doi:10.3238/arztebl.2018.0646
- Thomas A, Necchi A, Muneer A et al. Penile cancer. Nat Rev Dis Primers. 2021; 7(1): 11. doi:10.1038/s41572-021-00246-5
- Daling JR, Madeleine MM, Johnson LG et al. Penile cancer: Importance of circumcision, human papillomavirus and smoking in in situ and invasive disease. Int. J. Cancer 2005; 116(4): 606-616. doi:10.1002/ijc.21009
- Albero G, Villa LL, Lazcano-Ponce E et al. Male circumcision and prevalence of genital human papillomavirus infection in men: a multinational study. BMC Infect Dis. 2013; 13(1). doi:10.1186/1471-2334-13-18
- De Martel C, Plummer M, Vignat J et al. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int J Cancer. 2017; 141: 664-670.
- NCCN Guidelines Version 2.2020 Penile Cancer.
- Tang V, Clarke L, Gall Z et al. Should centralized histopathological review in penile cancer be the global standard? BJU Int. 2014; 114(3): 340-343.
- NCCN Guidelines Version 2.2020 Penile Cancer.
- Raskin Y, Vanthoor J, Milenkovic U, Muneer A, Albersen M. Organ-sparing surgical and nonsurgical modalities in primary penile cancer treatment. Curr Opin Urol. 2019; 29: 156-164.
CONFLICT OF INTEREST STATEMENT
The authors of this article declare that they have no conflict of interest with respect to what is expressed in this work.
Luisa Fernanda Sánchez Musi
Urology Department of Mexico General Hospital “Dr. Eduardo Liceaga”
Mexico Anahuac University, School of Medicine
Tlf.: +52 558 532 9000 | E-Mail: Luisa.sanchezmu@anahuac.mx
Año 2022 · número 137 (02) · páginas 194 a 199
Enviado: 23.06.22
Revisado: 29.06.22
Aceptado: 12.07.22