Abstract
The fields of population movement (migration) and health inequity are hugely complex each in their own rights with numerous intricate theoretical models as well as practical and political implications. Integrating the two only multiplies the number of variations. Migration patterns vary in terms of whether they have slow or rapid onset, the cause is human/political or natural, the direction is unidirectional or circular and whether it is voluntary or forced.
Health inequity operates through mechanisms at various levels such as socio-economic context and position, differential exposure, differential vulnerability, differential outcome, and differential consequences. Therefore, this article is an analysis of social determinants linked to migration in the context of the Social Development Goals for 2030.
In this article, structured as a narrative review, the two conceptual frameworks will be juxtaposed in order to provide guidance to public health planning and research for migrant populations and address global health inequities. Taking three diseases (visceral leishmaniasis, diabetes mellitus and tuberculosis) as exemplary cases, it is shown how various sorts of migration patterns may aggravate health inequity in various ways.Resumen
Los ámbitos que abarca el movimiento poblacional (migración) y la inequidad en salud son enormemente complejos en sí mismos, con numerosos modelos teóricos intrincados, así como con muchas implicaciones prácticas y políticas. La integración de ambos –migración e inequidad- multiplica exponencialmente las variaciones posibles.
Los patrones migratorios varían según si su inicio es lento o rápido, si la causa es humana/política o natural, si la dirección es unidireccional o circular, y si se trata de una migración voluntaria o forzada.
La inequidad en salud opera a través de mecanismos a distintos niveles, como el contexto y la posición socioeconómica, la exposición diferencial, la vulnerabilidad diferencial, los resultados diferenciales y las consecuencias diferenciales. Consiguientemente, este trabajo es un análisis de los determinantes sociales asociados a la migración en el contexto de los Objetivos del Desarrollo Sostenible para el 2030.
En este artículo, estructurado como una revisión narrativa, se yuxtaponen ambos marcos conceptuales con el objetivo de ofrecer orientación para la planificación en salud pública y la investigación en poblaciones migrantes, y abordar las inequidades en salud a nivel global. Tomando tres enfermedades (leishmaniasis visceral, diabetes mellitus y tuberculosis) como ejemplos, se demuestra cómo diferentes tipos de patrones migratorios pueden agravar la inequidad en salud de diversas maneras.Keywords: Conceptual framework; Diabetes mellitus; Health inequity; Migration; Tuberculosis; Visceral leishmaniasis.
Palabras clave: Marco conceptual; Diabetes mellitus; Inequidad en salud; Migración; Tuberculosis; Leishmaniasis visceral.
1. INTRODUCTION
This article brings together two topical themes – migration and health inequity. Both topics are highly complex in their own right, and the combination of the two adds even further to the complexity. The global trend in involuntarily displaced populations has continued to increase (1), though it is essential to remember, that there are many other sorts of population movement such as education, labor, and family unification (2). Although the importance of social determinants of health have been recognized for a long time, the more recent contribution of the Commission of the Social Determinants of Health (CSDH) provided further evidence as well as political attention (3). Recent reviews have provided updated overviews of the complexity of the field globally as well as in the European region (4,5,6,7,8).
This article will juxtapose two conceptual frameworks from the fields of migration and health inequity respectively to guide public health planning and research.
2. Methodology
This study is based on a narrative review, aimed at providing a comprehensive overview of the intersection between conceptual frameworks of migration and health inequity, allowing for a broader and more flexible exploration of available information, and facilitating the integration of multiple theoretical and contextual perspectives.
To identify relevant literature, a search was conducted in academic databases using the following key terms: Conceptual framework, health inequity, migration, tuberculosis, visceral leishmaniasis, diabetes mellitus. Studies addressing the relationship between migration patterns and health inequities were reviewed, with a particular focus on the three diseases considered exemplary cases in this analysis.
The reviewed literature was assessed according to its relevance to the study’s conceptual framework, prioritizing research that contributed empirical evidence, theoretical models, or public health policy analyses. This approach allowed for the identification of connections between the various mechanisms through which migration influences health inequity and the development of an integrated perspective to guide public health planning and research.
3. Patterns of migration
The United Nation’s International Organization for Migration (IOM) (2022) (1,4) defines a “migrant with an umbrella term, not defined under international law, reflecting the common lay understanding of a person who moves away from his or her place of usual residence, whether within a country or across an international border, temporarily or permanently, and for a variety of reasons”. This is not a globally recognized term, but it guides the work of the organization. The IOM (2022) estimates that the “number of international migrants has increased over the past five decades.
The total estimated 281 million people living in a country other than their countries of birth in 2020 was 128 million more than in 1990, and over three times the estimated number in 1970” (1,4,5).
Recent years’ large waves of population movement (e.g. from Ukraine and Palestine to neighboring countries due to the recent wars, from Africa and the Middle East to Europe, and from Latin America to Central and North America and other countries) are conspicuous examples of migration with detrimental health effects and other negative consequences – either driven by forced and rapid refuge from immediate danger, or more protracted flows of migrants converging towards regions with presumed better economic potential. Notwithstanding the importance of these tragic events, it should be borne in mind that there are many other sorts of population movements (1,4,5).
A comprehensive framework of population movements has been suggested based on work by previous scholars (Table 1) (2). This conceptual framework displayed the multitude of forms in which population movement takes place according to the variables of ‘onset’ (slow or rapid), ‘cause’ (human/political or natural), ‘direction’ (unidirectional or circular) and ‘motivation’ (voluntary or forced). Overall, the table displays the many different sorts of population movement.
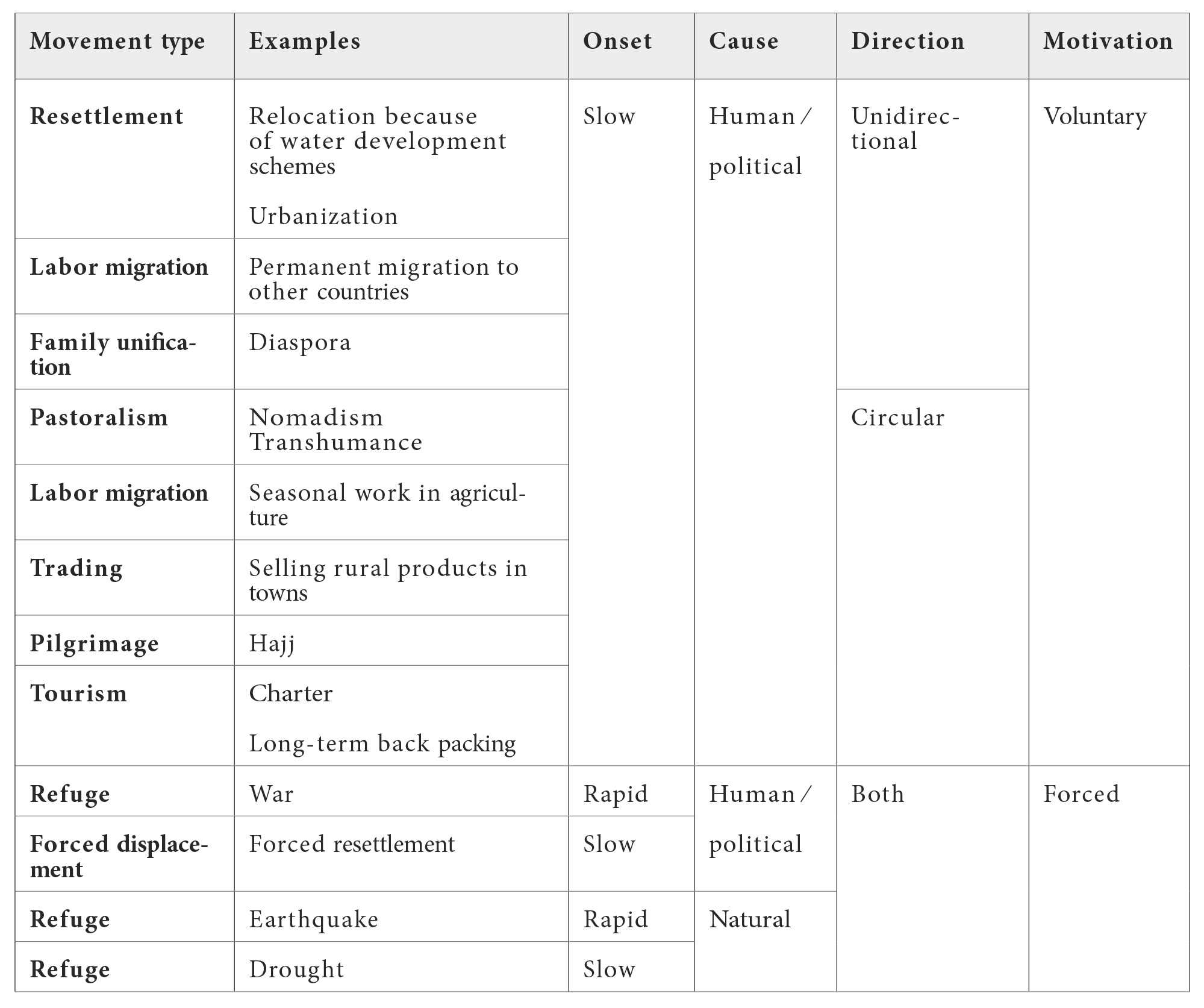
Despite its complexity, this framework is still an over-simplification, and the individual categories are not absolutely distinct. For instance, labor migration may be intended to be temporary, but turns out to be permanent or vice versa. Furthermore, recent developments have shown that the distinction between human/political and natural may not always be clear (9), and refuge due to natural causes has also been caused by rising sea levels (10,11). The concept of ‘mixed migration flows’ has also drawn the attention to the issue (12).
In short, this typology illustrates that population movements are multi-faceted and very complex (13). Furthermore, it should be pointed out that migration patterns should be analyzed in the local contexts. Thus, the degree of similarity between migrants and the host population in terms of language, ethnicity, traditions, or religion as well as previous historical ties or animosity play major roles.
4. Health inequity
The insight that there is more to ill-health than biology, is not new. In 1848, John Snow showed the causal relationship between polluted water from the Thames distributed by a water pump and an outbreak of cholera in the London quartier served by this pump (14). Shortly after, Rudolf Virchow (1821-1902) conducted his visionary work in the second half of the 1800 hundred, integrating disease in the social context, and he stated that “if medicine were to fulfil her great task, then it must enter the political and social life; therefore, medicine must be viewed as a social science” (15). In more recent times a number of outstanding scholars have further refined the theoretical foundations (16).
In its seminal report ‘Closing the gap in a Generation’, the CSDH made a strong case for the importance of health inequity based on social determinants of health (3). The commission used an analytical framework for causal pathways for health action including five levels allowing a differentiation of the ways in which the social determinants operate (3,17), which will be used in a simplified manner in this article:
- Socio-economic context and position focus on the societal organization and distribution of entitlements at the national level including models of health care funding or institutionalized discrimination against various groups.
- Differential exposure describes the likelihood of getting a disease either due to infection or living in unhealthy environments.
- Differential vulnerability is here perceived as whether individuals or groups have an increased risk of getting infected due to biomedical reasons such as co-morbidity or malnutrition, rather than the social meaning of the concept.
- Differential health care outcomes focus on the level of impact of the curative health care services.
- Differential consequences pertain to the situation after concluded treatment, e.g., economically (3,17).
The CSDH used the framework to differentiate between various levels such as individual, population group and society and to identify causal links between them. In the present article, this analytical framework will be applied in a simplified form where the five levels individually allow to differentiate the ways in which the social determinants operate (3). The CSDH (2008) report was supplemented by a number of preparatory reports (16-17) and work focusing on specific public health programs (18). Graham (2004) pointed out that it is important to distinguish between determinants of health and determinants of health inequities, and the present article focuses on the former (19).
Health care services have been identified as a social determinant of health in their own right (16) and deserves particular attention. The quality of the health care services is essential to differential outcomes. Based on the work of previous scholars, we will use the following elements of coverage: availability, accessibility, affordability, acceptability, and adherence (20,21). In short, there are several reasons why patients may not benefit from the required health care services and thereby achieve the desired ‘outcome’.
5. Disease cases
In this section we display three exemplary disease cases (visceral leishmaniasis, diabetes mellitus and tuberculosis) which in various ways illustrate the issues. These have been selected to cover non-communicable as well as (semi-acute and chronic) communicable diseases.
5.1. Visceral leishmaniasis
Visceral leishmaniasis (VL) is a protozoan, vector-borne disease transmitted by sandflies and grouped among the neglected tropical diseases (NTDs). VL is present in 80 countries. If in 2006 67% of the cases were in South Asia and 17% in East Africa, today figures inverted to 12% and 60%, respectively, due to a successful elimination program in the former (22–23).
Poor environmental sanitation increases sandfly density near infected reservoirs such as humans or dogs. Environmental variables such as temperature, soil type and vegetation coverage are the most important ecological determinants of the distribution of leishmaniasis vectors (24). Host susceptibility plays a major role in transmission, being either herd or individual, acquired or natural, or based on immunosuppression or co-morbidity.
VL is anthroponotic (i.e. transmitted from person to person) in the South Asia and East Africa regions, while it is zoonotic (transmitted via infected animal reservoirs) in Brazil, the Mediterranean basin, and Central Asia where dogs are the main reservoir. Anthroponotic VL may potentially be controlled and eliminated as a public health problem. Elimination of zoonotic VL is a more complex problem since canids and other mammals constitute reservoirs. Dogs are asymptomatic in more than 50% of the infected cases and highly infective to sandflies, and they can walk up to 40 km per day (25).
Fatal if untreated, VL is closely linked to poverty and commonly transmitted in remote areas with fragmentary access to health care (26). The current anti-VL drug choices are still limited and have adverse effects, toxicity, high cost and poor efficacy. Furthermore, they need multiple injection and are prone to drug resistance.
Several forms of population movement are responsible for the increase of VL incidence (27). In an analysis comprising the period 1995-2010, wars and political terror have been associated with a six folds increase of VL, directly related to health system disruption (28). In anthroponotic VL, civil unrest and wars impose major flows of naïve and probably malnourished population groups into endemic areas causing outbreaks and a disproportionally high mortality up to 30% (29). If returning to their place of origin the disease spreads to new areas, taking into account that the sandfly is globally present in various degrees (30).
Labor migration is also well described as a reason for major outbreaks of VL. In Ethiopia, highlanders migrate to the more fertile lowlands in Tigray every year for harvesting sesame and sorghum, where they live in crowed shelters during several months being exposed to the bites of sandflies in a highly endemic area (31). It has been shown, that upon return the labor migrants have caused a major outbreak in the highlands, an area free from leishmaniasis previously (32). In South Sudan where the most important outbreaks happen regularly counting by thousands the patients in each epidemic, the establishment of sentinel sites, some in the expected corridors of migration, reduced the mortality from 30% to less than 4% among more than 20,000 patients (33).
In Latin America, especially Brazil and northern Argentina, VL is undergoing a twofold urbanization process. Either the rural population migrates to the periphery of cities in contact with the forest where leishmaniasis is transmitted, or humans invade the forest provoking environmental degradation facilitating bringing humans closer to vector-breeding sites and facilitating vector adjustment to peri-domestic habitats (34).
5.2. Diabetes mellitus
Diabetes mellitus (DM) is a chronic, endocrine disease caused by inadequate production of insulin in the pancreas and/or ineffective use of the hormone, which leads to increased blood glucose. It is estimated that 537 million adults lived with DM in 2021 out of whom 75% lived in Low-and Middle-Income Countries. The annual mortality due to DM was 6.7 million deaths that same year (35).
The two main variants of DM are types 1 and 2. The former has a sudden onset typically in childhood or youth with need of insulin injections from the start. The latter, which constitutes 95% of all cases, has a more gradual course and frequently remains undiagnosed. Type 2 DM mostly occurs later in life and is often manageable with oral medication. Both types of DM require healthy dietary practices and adequate physical activity and benefit from maintenance of normal weight. The main challenges are vascular or neural complications potentially leading to blindness, foot ulcers and potentially loss of limbs, kidney dysfunction and major cardio-vascular events such as strokes or heart attacks. Especially when not controlled appropriately, DM may increase susceptibility to various infectious diseases (36).
Irrespectively of the type, a person with DM depends on a stable supply of drugs such as insulin or metformin, and quite often additional treatment for hypertension and elevated blood fats. Apart from the drugs themselves, optimal diabetes care also includes access to blood glucose monitoring and to qualified staff who can advise on dosage and screen for renal, ophthalmological, and neural complications. Though this is the ideal, it admittedly rarely happens even among non-migrating populations, and quality of DM control of blood sugar and hypertension is inversely associated with the national levels of economic development. This trend is less pronounced but still existent in countries with universal and therefore affordable health care. Similar disparages are found for DM-related complications and mortality in various countries (37).
National health care systems usually find it difficult to cater for pastoral groups with no fixed residential location even within a given country leading to reduced health outcomes. Population segments forced to take sudden refuge either due to natural disasters or human/political reasons, may find themselves in neighboring countries without nearby health care facilities, leave alone entitlement to the services provided within the local socio-economic context and this may subsequently lead to disparities in health outcomes or consequences. The same goes for the flows of migrants often crossing several countries and sometimes oceans in order to reach more affluent parts of the world such as United States of America (USA) or the European Union (37).
5.3. Tuberculosis
Tuberculosis (TB) is a communicable disease caused by the bacillus Mycobacterium tuberculosis. An estimated 10.6 million people fell ill with TB worldwide in 2021, equivalent to 134 cases per 100,000 population (38). It is present in all countries and age groups. A total of 90% of the TB cases are adults, with more men than women being affected. TB mostly affects the lungs based on transmission by droplets from person to person, but there is also a bovine form spread by contaminated milk (39).
The death rate is about 50% in manifest TB without treatment. However, about 85% of the patients can be cured with the currently recommended standard treatment (4-6 months course of a combination of anti-TB drugs). Some strains of the TB bacillus have developed resistance to the commonly prescribed drugs (DR), which is a public health threat of great concern.
In addition to contagion, DR-TB occurs when drugs for proper treatment are not available or they have poor quality, health care providers prescribe the wrong dosage, or the patients do not complete a full course of treatment. An important problem for adherence to DR-TB treatment is the serious side effects as well as the higher cost (40). DR-TB is categorized into five categories of increasing severity according to the number of drugs (39).
Migrants from countries with high TB incidence are the dominant group of people with active TB disease in many recipient countries (41). Foreign-born migrants contribute to the burden of TB with an increasing number of newly diagnosed cases in many high-income countries (39). Re-activation of latent TB infection among migrants in Europe has driven national policies for identifying and treating latent TB infection among them to reduce TB incidence (42).
More than 50% of previously treated cases with severe DR-TB in 2021 have been found in the Russian Federation, Central Asia, and Eastern Europe (30), and migrants from Eastern Europe have a higher degree of multi-DR than other regions like sub-Saharan Africa (43–44).
Long and expensive treatment regimens for TB together with economic barriers can affect access to health care for diagnosis and completion of treatment (outcomes), with catastrophic total costs for migrants and their families (consequences) (45).
The World Health Organization (WHO) suggests that improving TB care among migrants should be considered as a key public health priority towards elimination of TB, and the multi-pronged ‘End TB strategy’ includes universal access to hygiene and infection control measures and cross-border care as priorities (39,46).
6. Integrating migration and health inequity perspectives
VL and TB are both communicable diseases requiring relatively long-term treatment regimens, though VL has a more acute progression. In contrast, DM is a non-communicable, chronic condition requiring life-long health care. Table 2 summarizes how the three disease cases exemplify the ways in which various sorts of migration patterns may aggravate the health inequities based on various mechanisms.
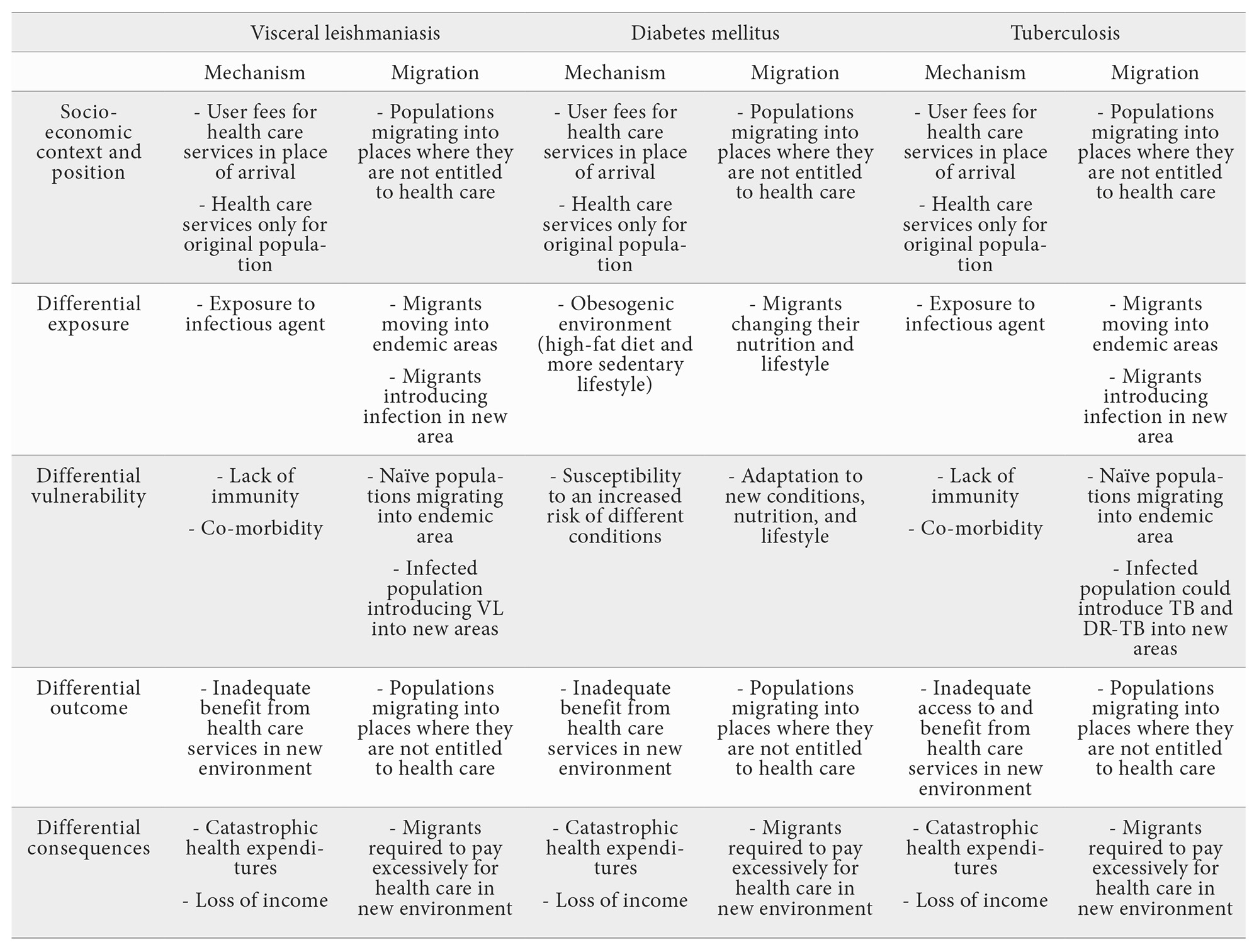
The social determinants of health, which encompass economic, environmental, and sociopolitical factors, shape health inequity affecting the well-being of populations. All the three cases share characteristics at the levels of socio-economic context and position, differential outcome, and consequences. These are to a large extent related to the health care services. In the case of migrants, the inequity is exacerbated by structural barriers that limit their access to essential resources, such as adequate housing, stable employment, and proper healthcare. Adequate access to local health care services (in the broad sense of the word including availability, affordability, and acceptability) for the migrants poses a challenge in relation to all three diseases. There is an important variability between countries regarding health policies and health-care access for migrants (8). As many governments find it hard to cater for the health care needs even of ‘their own’ stationary populations, the migrants from abroad are likely to face additional problems. This issue is closely related to how the national health authorities have organized the funding (socio-economic context and position). If the migrants fall sick in an environment where services are paid for directly by the patients, they may face situations of differential consequences such as catastrophic health expenditures, and this apply to all three disease cases.
In addition to the health inequity mechanisms mentioned above, there are additional issues at stake for the two infectious diseases (VL and TB). In these cases, migration often leads to increased risk of infection (differential exposure). For instance, migration populations may enter areas endemic for disease with which they are not used, or the migrants may introduce new pathogens to the stationary populations at arrival. In some cases, the migrants bring their domestic animals which may serve as reservoirs (e.g. dogs for VL) (47). In relation to exposure, the level of differential vulnerability may also play a role due to either lack of immunity or co-morbidities with a propensity of reducing the resilience. Additionally, there may be a delay in diagnosis among migrants due to fear of losing their job, fear of stigma and discrimination, and their intention to protect their contacts and family (in the case of TB). This can lead to migrants hiding their symptoms and not going to a health center, increasing the risk of non-detection and transmission (48).
To add further to the complexity, the local context plays a key role. Thus, the combination of local languages, ethnicities, traditions and religions make a major difference. Evidently, migration between two countries with very similar conditions reduce the challenges – everything being equal. However, many migrants may have experienced poverty, which could have conditioned their bodies to cope with hunger and scarcity. Poverty plays a central role in this process, functioning as a cross-cutting determinant that amplifies vulnerabilities and restricts the ability of affected populations to adopt preventive measures or access timely treatments. Consequently, when they move to new countries with environments conducive to weight gain, characterized by high-fat diets and low physical activity, they are particularly susceptible to an increased risk of conditions such as DM. Interestingly, once these migrants gain stability in their new communities, their children also often experience higher rates of DM. This is sometimes seen as a result of their families’ adaptation to their new surroundings (49–50). At the other extreme, migrants with different languages and maybe even arriving among hostile populations with antagonistic ethnicities and/or religions may aggravate the situation.
From a global perspective, these challenges must be addressed within the framework of the Sustainable Development Goals (SDGs), which emphasize the need to reduce inequalities (SDG 10), ensure health and well-being for all (SDG 3), and promote more inclusive societies (SDGs 1 and 8). Adopting an approach aligned with the SDGs allows for understanding health inequity not only as a consequence of migration and poverty, but also as a reflection of broader exclusionary structures that perpetuate unequal access to fundamental rights.
7. Conclusion
A typology for population movement categorized the many varieties according to onset (slow or rapid), cause (human/political or natural), direction (unidirectional or circular) and motivation (voluntary or forced) (2). The CSDH applied an analytical framework, which distinguished between disparities at the levels of society, exposure, vulnerability, outcome, and consequences at which health inequity could come into play (3). Common for the two approaches is that they deconstruct the notions of migration and health inequity according to a more detailed set of variables and, as such, this paper contributes for a better understanding of the social determinants linked to migration to be considered for targeting the 2030 SDGs.
This article does not aim to provide comprehensive reviews of these two main concepts. Instead,it illustrates how the juxtaposition of the two analytical perspectives enables a more in-depth analysis of migration and health inequity. The aim is that this dual conceptual framework will guide future public health planning and research in their endeavor to navigate the complex challenges of global health inequities.
Acknowledgements
We are thankful to our many colleagues from whom we have learned over the years.
Funding
N/A.
Conflicts of interest
The authors of this article declare that they have no conflict of interest with respect to what is expressed in this work.
BIBLIOGRAPHY
- ↑United Nation’s International Organization for Migration (IOM). https://www.iom.int. Accessed 19 Dec 2023.
- ↑Aagaard-Hansen J, Nombela N, Alvar J. Population movement: a key factor in the epidemiology of neglected tropical diseases. Trop Med Int Heal. 2010; 11:1281–1288. https://onlinelibrary.wiley.com/doi/10.1111/j.1365-3156.2010.02629.x.
- ↑World Health Organization. Closing the gap in a generation. Commission on Social Determinants of Health (CSDH). Geneva: World Health Organization; 2008. http://www.bvsde.paho.org/bvsacd/cd68/Marmot.pdf%5Cnpapers2://publication/uuid/E1779459-4655-4721-8531-CF82E8D47409.
- ↑McAuliffe, M. and A. Triandafyllidou (eds.), 2021. World Migration Report 2022. International Organization for Migration (IOM), Geneva.
- ↑Internal Displacement Monitoring Centre (IDMC), & Norwegian Refugee Council. (2023). Global Report on Internal Displacement (2023): Internal displacement and food security. Https://Api.Internal-Displacement.Org/Sites/Default/Files/Publications/Documents/IDMC_GRID_2023_Global_Report_on_Internal_Displacement.
- ↑Abubakar I, Aldridge RW, Derakumar D et al. The UCL-Lancet Commission on Migration and Health: the health of a world on the move. Lancet 2018.;392(10164):2606-2654.
- ↑Marmot M, Allen J, Bell R, Bloomer E, Goldblatt P; Consortium for the European Review of Social Determinants of Health and the Health Divide. WHO European review of social determinants of health and the health divide. Lancet. 2012 ;380(9846):1011-1029. doi: 10.1016/S0140-6736(12)61228-8. Epub 2012 Sep 8. PMID: 22964159.
- ↑Lebano A, Hamed S, Bradby H, et al. Migrants’ and refugees’ health status and healthcare in Europe: a scoping literature review. BMC Public Health. 2020 ;20(1):1039. doi: 10.1186/s12889-020-08749-8. PMID: 32605605; PMCID: PMC7329528.
- ↑Castelli F. Drivers of migration: why do people move? J Travel Med. 2018;25(1):1–7. https://academic.oup.com/jtm/article/doi/10.1093/jtm/tay040/5056445.
- ↑Bellizzi S, Popescu C, Panu Napodano CM, Fiamma M, Cegolon L. Global health, climate change and migration: The need for recognition of “climate refugees”. J Glob Health. 2023 Mar 24; 13:03011. doi: 10.7189/jogh.13.03011. PMID: 36960688; PMCID: PMC10037158.
- ↑McMichael C, Dasgupta S, Ayeb-Karlsson S, Kelman I. A review of estimating population exposure to sea-level rise and the relevance for migration. Environ Res Lett. 2020 Dec;15(12):123005. doi: 10.1088/1748-9326/abb398. Epub 2020 Nov 27. PMID: 34149864; PMCID: PMC8208600.
- ↑Degani P, De Stefani P and Freedman J Editorial: Mapping vulnerability amid mixed migration flows. The reality of severe labor exploitation from a human rights perspective. Front. Hum. Dyn.2022; 4:1073606. doi: 10.3389/fhumd.2022.1073606.
- ↑Hossin MZ. International migration and health: it is time to go beyond conventional theoretical frameworks. BMJ Glob Health. 2020 ;5(2): e001938. doi: 10.1136/bmjgh-2019-001938. PMID: 32180999; PMCID: PMC7053782.
- ↑Bingham P, Verlander NQ, Cheal MJ. John Snow, William Farr and the 1849 outbreak of cholera that affected London: a reworking of the data highlights the importance of the water supply. Public Health. 2004;118(6):387–394. https://linkinghub.elsevier.com/retrieve/pii/S0033350604001106.
- ↑Dunn L. Rudolf Virchow. Four Lives in One. Wroclaw: Amazon Fulfillment; 2016. pp.1–285.
- ↑Solar O, Irwin A. A conceptual framework for action on the social determinants of health. Social determinants of health discussion. Paper 2 (Policy and practice). Geneva; 2010. http://apps.who.int/iris/bitstream/handle/10665/44489/9789241500852_eng.pdf?sequence=1.
- ↑Whitehead M, Dahlgren G. Levelling up (part 1): a discussion paper on concepts and principles for tackling social inequities in health. Copenhagen: WHO Regional Office for Europe; 2006.
- ↑Blas, E, Kurup AS. (Editors) Equity, social determinants, and public health programmes. Geneva: World Health Organization. 2010. https://apps.who.int/iris/handle/10665/44289.
- ↑Graham H. Social Determinants and Their Unequal Distribution: Clarifying Policy Understandings. Milbank Q. 2004;82(1):101–124. https://onlinelibrary.wiley.com/doi/10.1111/j.0887-378X.2004.00303.x.
- ↑Tanahashi T. Health service coverage and its evaluation. Bull World Health Organ. 1978;56(2):295–303. https://apps.who.int/iris/handle/10665/261736.
- ↑Tugwell P, de Savigny D, Hawker G, Robinson V. Applying clinical epidemiological methods to health equity: the equity effectiveness loop. BMJ. 2006;332(7537):358-361. https://www.bmj.com/lookup/doi/10.1136/bmj.332.7537.358.
- ↑Alvar J, Beca-Martínez M, Argaw D, Saurabh J, Aagaard J. Social determinants of visceral leishmaniasis elimination in Eastern Africa. BMJ Glob Health 2023;8:e012638. doi:10.1136/ bmjgh-2023-012638.
- ↑Alvar J, Vélez ID, Bern C, et al. Leishmaniasis Worldwide and Global Estimates of Its Incidence. PLoS One. 2012;7(5): e35671. https://dx.plos.org/10.1371/journal.pone.0035671.
- ↑>Gadisa E, Tsegaw T, Abera A, Elnaiem D, den Boer M. Eco-epidemiology of visceral leishmaniasis in Ethiopia. Parasit Vectors. 2015;1–10. http://dx.doi.org/10.1186/s13071-015-0987-y.
- ↑Alvar J, Cañavate C, Molina R, Moreno J, Nieto J. Canine Leishmaniasis. Adv Parasitol. 2004; 57:1–88. https://doi.org/10.1016/s0065-308x(04)57001-x.
- ↑Alvar J, Yactayo S, Bern C. Leishmaniasis and poverty. Trends Parasitol. 2006;22(12):552–557. https://linkinghub.elsevier.com/retrieve/pii/S147149220600239X.
- ↑Alvar J, den Boer M, Dagne DA. Towards the elimination of visceral leishmaniasis as a public health problem in east Africa: reflections on an enhanced control strategy and a call for action. Lancet Glob Heal. 2021;9(12): e1763–9. http://dx.doi.org/10.1016/S2214-109X(21)00392-2.
- ↑Berry I, Berrang-Ford L. Leishmaniasis, conflict, and political terror: A spatio-temporal analysis. Soc Sci Med. 2016; 167:140–149. https://linkinghub.elsevier.com/retrieve/pii/S0277953616302210.
- ↑Seaman J, Mercer AJ, Sondorp E. The epidemic of visceral leishmaniasis in western Upper Nile, southern Sudan: course and impact from 1984 to 1994. Int J Epidemiol. 1996;25(4):862–871. https://academic.oup.com/ije/article-lookup/doi/10.1093/ije/25.4.862.
- ↑Collin S, Davidson R, Ritmeijer K, et al. Conflict and Kala‐Azar: Determinants of Adverse Outcomes of Kala‐Azar among Patients in Southern Sudan. Clin Infect Dis. 2004;38(5):612–619. https://academic.oup.com/cid/article-lookup/doi/10.1086/381203.
- ↑Argaw D, Mulugeta A, Herrero M, et al. Risk Factors for Visceral Leishmaniasis among Residents and Migrants in Kafta-Humera, Ethiopia. PLoS Negl Trop Dis. 2013;7(11): e2543. https://dx.plos.org/10.1371/journal.pntd.0002543.
- ↑Alvar J, Bashaye S, Argaw D, et al. Kala-azar outbreak in Libo Kemkem, Ethiopia: epidemiologic and parasitologic assessment. Am J Trop Med Hyg. 2007;77(2):275–282. http://www.ncbi.nlm.nih.gov/pubmed/17690399.
- ↑Abubakar A, Ruiz-Postigo JA, Pita J, et al. Visceral Leishmaniasis Outbreak in South Sudan 2009–2012: Epidemiological Assessment and Impact of a Multisectoral Response. PLoS Negl Trop Dis. 2014;8(3): e2720. https://dx.plos.org/10.1371/journal.pntd.0002720.
- ↑Harhay MO, Olliaro PL, Costa DL, Costa CHN. Urban parasitology: visceral leishmaniasis in Brazil. Trends Parasitol. 2011;27(9):403–409. https://linkinghub.elsevier.com/retrieve/pii/S147149221100064X.
- ↑International Diabetes Federation (IDF). IDF Diabetes Atlas. 2023. https://diabetesatlas.org. Accessed 24 Jan 2023.
- ↑World Health Organizaton. Fact sheets on diabetes. 2023. https://www.who.int/news-room/fact-sheets/detail/diabetes. Accessed 10 Jun 2022.
- ↑Whiting D, Unwin N, Roglic G. Diabetes: equity and social determinants. In: Equity, social determinants and public health programmes. In: E Blas and AS Kurup (Editors): Equity, social determinants and public health programmes. Geneva: World Health Organization. 2010. pp.77-94. https://apps.who.int/iris/handle/10665/44289.
- ↑World Health Organization. Global Tuberculosis Report 2022. TB incidence. 2022. https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2022/tb-disease-burden/2-1-tb-incidence. Accessed 10 Jun 2022.
- ↑World Health Organization. Global tuberculosis report 2022. 2022. https://www.who.int/teams/global-tuberculosis-programme/tb-reports. Accessed 10 Jun 2022.
- ↑Centers for Disease Control and Prevention. Drug-Resistant TB. 2022. https://www.cdc.gov/tb/topic/drtb/default.htm. Accessed 10 Jun 2022.
- ↑Lönnroth, K, Jaramillo, E, Williams, B, Chris D and RM. Tuberculosis: the role of risk factors and social determinants. In: E Blas and AS Kurup (Editors): Equity, social determinants and public health programmes. Geneva: World Health Organization. 2010. pp.219–242. https://apps.who.int/iris/handle/10665/44289.
- ↑Baggaley RF, Zenner D, Bird P, et al. Prevention and treatment of infectious diseases in migrants in Europe in the era of universal health coverage. Lancet Public Heal. 2022;7(10): e876–84. http://dx.doi.org/10.1016/S2468-2667(22)00174-8.
- ↑Musa BM, Adamu AL, Galadanci NA, Zubayr B, Odoh CN, Aliyu MH. Trends in prevalence of multi drug resistant tuberculosis in sub-Saharan Africa: A systematic review and meta-analysis. PLoS One. 2017;12(9): e0185105. https://dx.plos.org/10.1371/journal.pone.0185105.
- ↑The Global Fund. Global Fund supported TB/MDR-TB programs in Eastern Europe and Central Asia – focus on Uzbekistan, Kyrgyzstan, and Tajikistan. 2022. https://www.theglobalfund.org/en/oig/updates/2022-08-26-audit-of-mdr-tb-programs-in-eastern-europe-and-central-asia/. Accessed 10 Jun 2022.
- ↑Woldesemayat EM. Tuberculosis in Migrants is Among the Challenges of Tuberculosis Control in High-Income Countries. Risk Manag Health Policy. 2021; 14:2965–2970. https://www.dovepress.com/tuberculosis-in-migrants-is-among-the-challenges-of-tuberculosis-contr-peer-reviewed-fulltext-article-RMHP.
- ↑WHO. Implementing the end TB strategy: the essentials. 2022. https://apps.who.int/iris/handle/10665/206499. Accessed 10 Jun 2022.
- ↑Fooks AR, Johnson N. Jet set pets: examining the zoonosis risk in animal import and travel across the European Union. Vet Med (Auckl). 2014; 6:17-25. doi: 10.2147/VMRR.S62059. PMID: 30101093; PMCID: PMC6067792.
- ↑Hayward S, Harding RM, McShane H, et al Factors influencing the higher incidence of tuberculosis among migrants and ethnic minorities in the UK. F1000Res 2028, 7: 461.
- ↑Montesi L, Caletti MT, Marchesini G Diabetes in migrants and ethnic minorities in a changing World. World J Diabetes.2016; 7: 34.
- ↑Maltoni G, Zioutas M, Mosticchio M, et al. A comparative study on the incidence of type 1 diabetes mellitus between children of North African migrants and Italian children in Emilia-Romagna region, Italy. Eur J Pediatr. 2022; 181: 1523–1529.
Jens Aagaard-Hansen
Faculty of Social Sciences and Humanities
Aalborg University (Copenhagen Campus), Denmark
Tlf.: +45 3030 1258 | E-Mail: jens@anthropology.dk
An RANM. 2025;142(01):11-20
Enviado: 12.01.25
Revisado: 18.01.25
Aceptado: 22.02.25