

Abstract
Background and Goal of Study: Blood salvage (BS) is important to implement the second pillar of Patient Blood Management to avoid anaemia after total knee arthroplasty (TKA). Our primary outcome was to assess BS usefulness to decrease allogenic blood transfusion (ABT) rate in TKA.
Materials and Methods: a retrospective, observational cohort study was conducted on consecutive patients scheduled for TKA with BS or not. Demographic, comorbidity, surgical and anesthetic data, laboratory pre and postoperative results, volume of blood drained, and reinfused from BS and the requirement of ABT were recorded. Parametric and non-parametric tests were employed. p< 0.05 was accepted as significant.
Results: 260 patients were included (130 per cohort). The amount of postoperative bleeding was 713.1 +445.4 ml. 26.5% received ABT. BS reduced transfusion in 13,1% (p=0,024) with RR 1,65 (CI 1,085-2,52)]. Risk factors for postoperative bleeding were: male gender, atrial fibrillation, preoperative anti-platelet therapy and cementless primary TKA. Risk factors for ABT: ASA > II, preoperative hemoglobin < 13 g/dl, knee revision, anti-platelet therapy, longer surgery time. Patients transfused had lower hemoglobin values (p<0.001), and longer medium LOS (+2.5 days, p=0.026).
Conclusion: The use of BS in TKA showed benefits reducing allogenic blood transfusion and length of hospital stay. BS would remain an effective, safe and cheap alternative to tranexamic acid in patients with high risk of thromboembolism events operated of TKA.Resumen
Introducción y Objetivo: El recuperador de sangre es un elemento importante del segundo pilar para la optimización de la anemia perioperatoria tras la artroplastia de rodilla (ATR). El objetivo principal de este estudio es determinar la eficacia de los recuperadores de sangre (RS) postoperatorios para reducir la tasa de transfusión de sangre alogénica (TSA) en el postoperatorio de la artroplastia de rodilla.
Material y Métodos: Se realizó un estudio retrospectivo de cohortes en pacientes intervenidos de ATR comparando el grupo en el que se utilizó RS y el grupo sin RS. Se recogieron y analizaron los datos demográficos, comorbilidad, información relevante de la cirugía y el procedimiento anestésico, resultados de laboratorio pre y postoperatorios, volumen de sangre recogido en el drenaje, volumen de sangre transfundido del RS y la necesidad de TSA. Se realizaron los test paramétricos y no paramétricos correspondientes. Se aceptó como nivel de significación estadística p<0,05.
Resultados: Se incluyeron 260 pacientes (130 por cohorte). La hemorragia postoperatoria fue de 713.1 +445.4 ml. El 26.5% recibió TSA. En la cohorte con RS la incidencia de TSA disminuyó un 13% (p=0,024) con RR 1,65 (CI 1,085-2,52). Se identificaron como factores de riesgo de hemorragia postoperatoria: género masculino, fibrilación auricular, terapia antiagregante y ATR no cementada. Los factores de riesgo de TSA identificados fueron: ASA > II, Hb preoperatoria <13 g/dl, recambio de rodilla, terapia antiagregante y tiempo quirúrgico prolongado. Los pacientes transfundidos presentaron cifras postoperatorias de Hb menores (p<0,001), y una estancia hospitalaria más prolongada (p=0,026).
Conclusión: El uso de los RS postoperatorios en la ATR es una medida eficaz para disminuir la TSA y la estancia hospitalaria. Los RS podrían ser una alternativa eficaz, segura y económica al uso de ácido tranexámico en aquellos pacientes con un riesgo elevado de eventos tromboembólicos intervenidos de ATR.Keywords: Operative Blood Salvage; Blood transfusion; Arthroplasty; Replacement; Knee; Anemia; Risk factors.
Palabras clave: Recuperadores de Sangre; Transfusión de Sangre; Artroplastia; Rodilla; Anemia; Factores de Riesgo.
INTRODUCTION
The incidence of arthritis and arthrosis is increasing at the same rate as the age and comorbidities of our population in high income countries. Consequently, the costs, risks and complications after total knee arthroplasty (TKA) are also on the rise (1).
Postoperative bleeding after TKA is one of the important outcomes to control, to avoid postoperative complications, especially in patients with comorbidity. Bleeding is greater during the first 6 postoperative hours and can reach up to 800 mL (2). Between 20 and 30% of patients undergoing major orthopedic surgery present moderate anemia, and an increased risk of requiring blood transfusion. For patients who undergo TKA, forty to fifty percent require allogenic blood transfusion (ABT) in the perioperative period (3). Transfusion complications have been widely recognized by many international organizations and commissions and include allergic reactions, transfusion-related acute lung injury (TRALI), ABO-incompatible transfusion and transfusion errors, infections, immunomodulation/suppression (4) and is associated with an increased risk of short and long term mortality (5).
In Europe, ETPOS (European Transfusion Practice and Outcome Study) group observed that restrictive transfusion protocols were used only in 63% of hospitals and blood salvage (BS) are used in 6% (6). BS is an important system to implement the second pillar of Patient Blood Management approach. Its advantages are its few adverse effects (2,7) pro-inflammatory effect minimizing the immunosuppression due to trauma and hemorrhage (8) and decreasing of the rate of ABT (9,10).
The use of BS has dropped markedly during the last years, due to the implantation of other techniques of perioperative patient blood management. The aim of this study was to assess the interest of BS for the improvement of the postoperative results of ABT and postoperative anaemia in a population of patients scheduled for a total knee arthroplasty.
MATERIALS AND METHODS
After having obtained the approval of our local Ethics Committee, a retrospective, observational cohort study was conduced in consecutive patients scheduled for TKA throughout twelve months in a tertiary university hospital. The medical data of all consecutive patients scheduled for TKA during that period were systematically reviewed. Inclusion criteria were to have undergone primary or replacement knee arthroplasty, excluding those in whom tranexamic acid (TXA) was administered by any routes available, and those for whom data collected was incomplete. The study was carried out on patients scheduled for TKA who were exposed to BS or not.
Demographic, comorbidity, surgical and anesthetic data were recorded until hospital discharge. Hematology and coagulation pre and postoperative results were collected at 6, 24, 48 hours and at hospital discharge from hospital. The volume of blood drained and reinfused from BS as well as the requirement of ABT were also recorded.
Primary outcome was to assess whether the use of BS postoperative reduced ABT, influenced hemoglobin and hematocrit levels and length of hospital stay (LOS). Secondary outcomes were to define risk factors for bleeding and receiving ABT after knee arthroplasty and to assess the influence of ABT on LOS.
After carrying out a preliminary study, the total incidence of ABT after knee arthroplasty was estimated to 23.3%. The sample size was calculated to 260 patients (130 per cohort), for a statistical power of 0.8 and an ⍺ error of 0.05 aiming at reducing ABT incidence by 50% and achieving an ABT incidence inferior or equal to 11.65% with the use of BS.
Statistical analysis was performed using SPSS version 11 /version 21 (SPSS Inc. Chicago. Illinois. USA®). Parametric and non-parametric tests were employed. Homogeneity of the two groups for pre-BS variables were checked. Comparisons between patients having or not received BS were carried out with One-Way and Two-Way Anova and Chi-Square tests. p< 0.05 was accepted as significant.
RESULTS
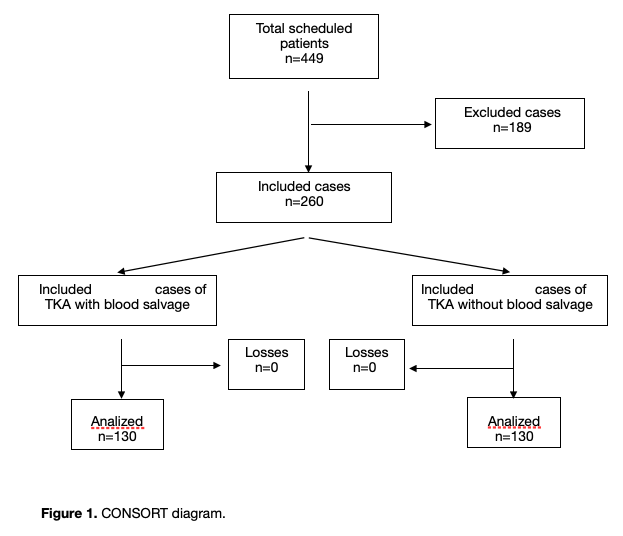
260 were included in the study, in 130 BS was used and in 130 BS was not used (figure 1, flow diagram). Homogeneity was checked for both groups for pre-BS variables (Table 1). The most frequent indication for surgery was osteoarthritis in 90.7% of cases. Primary TKA was performed in 91.5% (88.5% cemented, 1.5% cementless, 1.5% computer assisted TKA) and revision in 8.5%. Age was 71.69 +8.6 years. 67,9% of patients was ASA II classification and 29,3% was ASA III. Hypertension was the most common comorbidity (70,4%). 18,5% received preoperative anti-platelet therapy (APT) (Table 2).
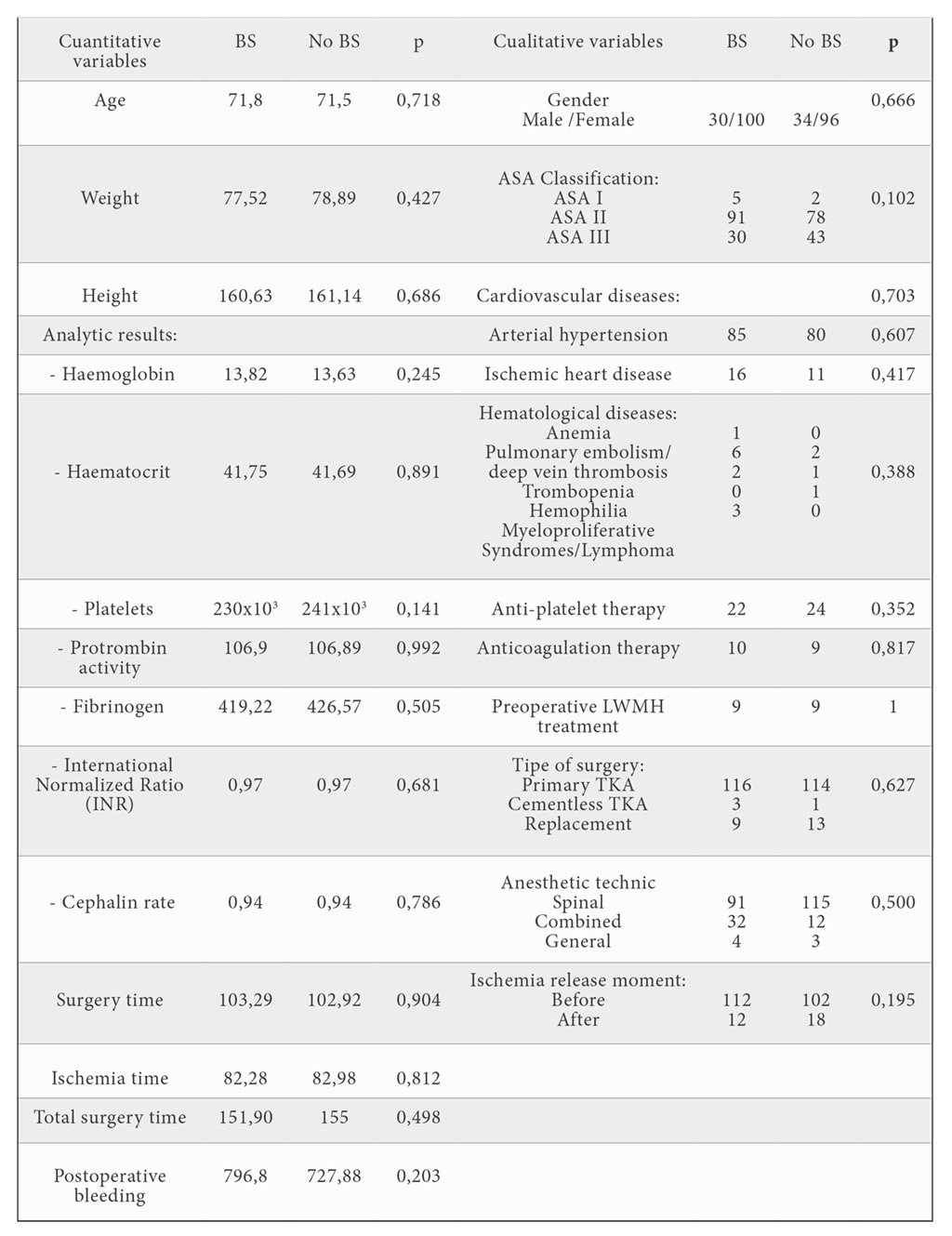
p: statistic signification. ANOVA.
BS: blood salvage; LWMH: low weigh molecular heparin; TKA: total knee arthroplasty.
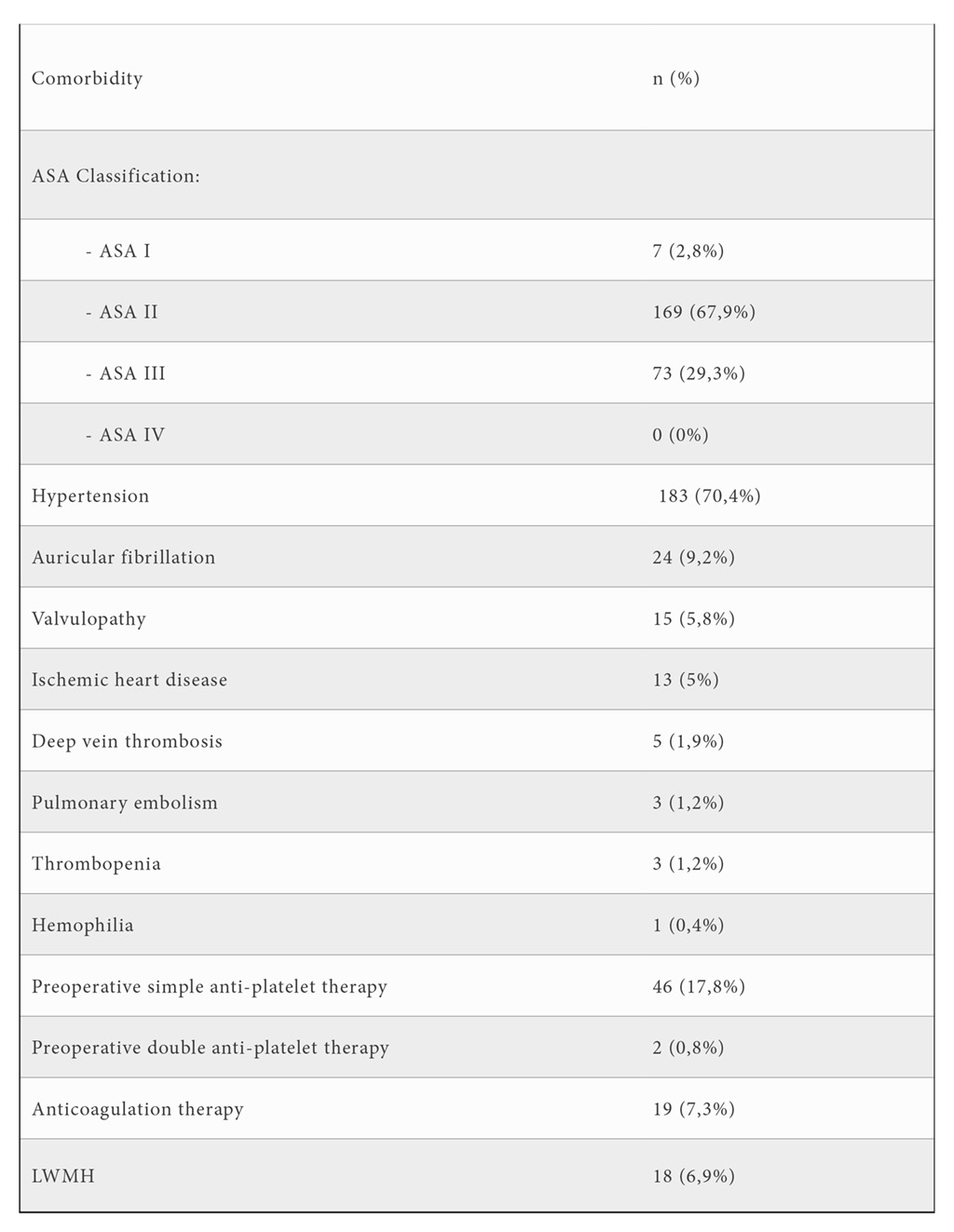
ASA Classification: American Society of Anesthesiologists Classification; LWMH: low weight molecular heparin.
Lower limb ischemia was used in 96,1% of cases, and in 84,3% was released before closing. Ischemia time was 82.62+22.7 min. Duration of surgery was 103,1+24,2 min. Loco-regional anesthesia was predominant used in 96.9% of cases, of which 79.5% were spinal anesthesia. Femoral block was the most frequent analgesic technique. General anesthesia was performed only in 3.1% of the cases. 93,5% of patients presented postoperative bleeding, mean bleeding volume was 713,1 +445,4 ml. In 90% of cases, recuperated blood was transfused, and the re-infused volume from BS was 619.96 +352.7 mL.
Dispite the existence of a Protocol for Preoperative Optimisation of Anaemia, this was not applied in all cases, resulting in 23.9% of patients who presented preoperative anaemia with hemoglobin levels (Hb) < 13 g/dL at the time of surgery. Only 2.4% had an Hb level < 11 g/dl being the lower Hb level 9.5 g/dl. Preoperative anaemia was significantly more prevalent in ASA (American Society of Anesthesiologists Classification) II and III patients (p=0,02). ABT prescription was guided by a Restrictive Transfusion Protocol (no patient receive packed red blood cells transfusion for Hb greater than 8 g/dL, or 10 mg/dL in cardiovascular risk patients, and that all of them were administered in one unit increments followed by re-evaluation of blood parameters). Patients who received ABT accounted for 26.5% of total cases, mainly in the late postoperative period (> 24 hours). 69.6% received 2 units of red blood cells and 11.6% received more than 2 units, equivalent to an average volume of 518.12+232.153 mL.
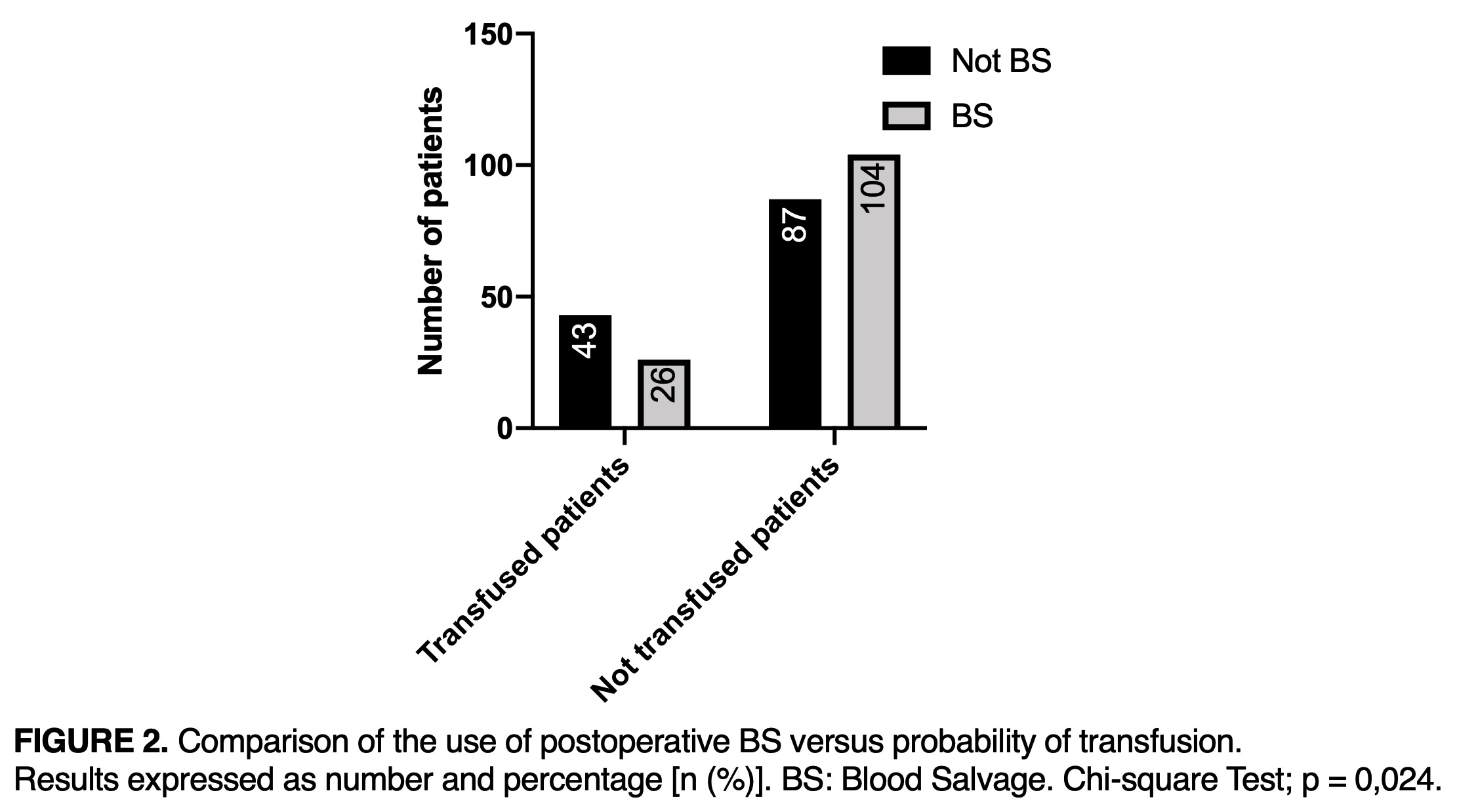
In the group without BS, 33.1% (43) patients received blood transfusion, versus 20% (26) in the group with BS exposed (OR: 95%CI 1.65 (CI 1.085-2.52); p=0.024). PACU time was 19.8 + 15.8 hours and the length of hospital stay (LOS) was 9.8 + 3.9 days (figure 2).
TKA: total knee arthroplasty; ASA Classification: American Society of Anesthesiologists Classification; p: statistic signification
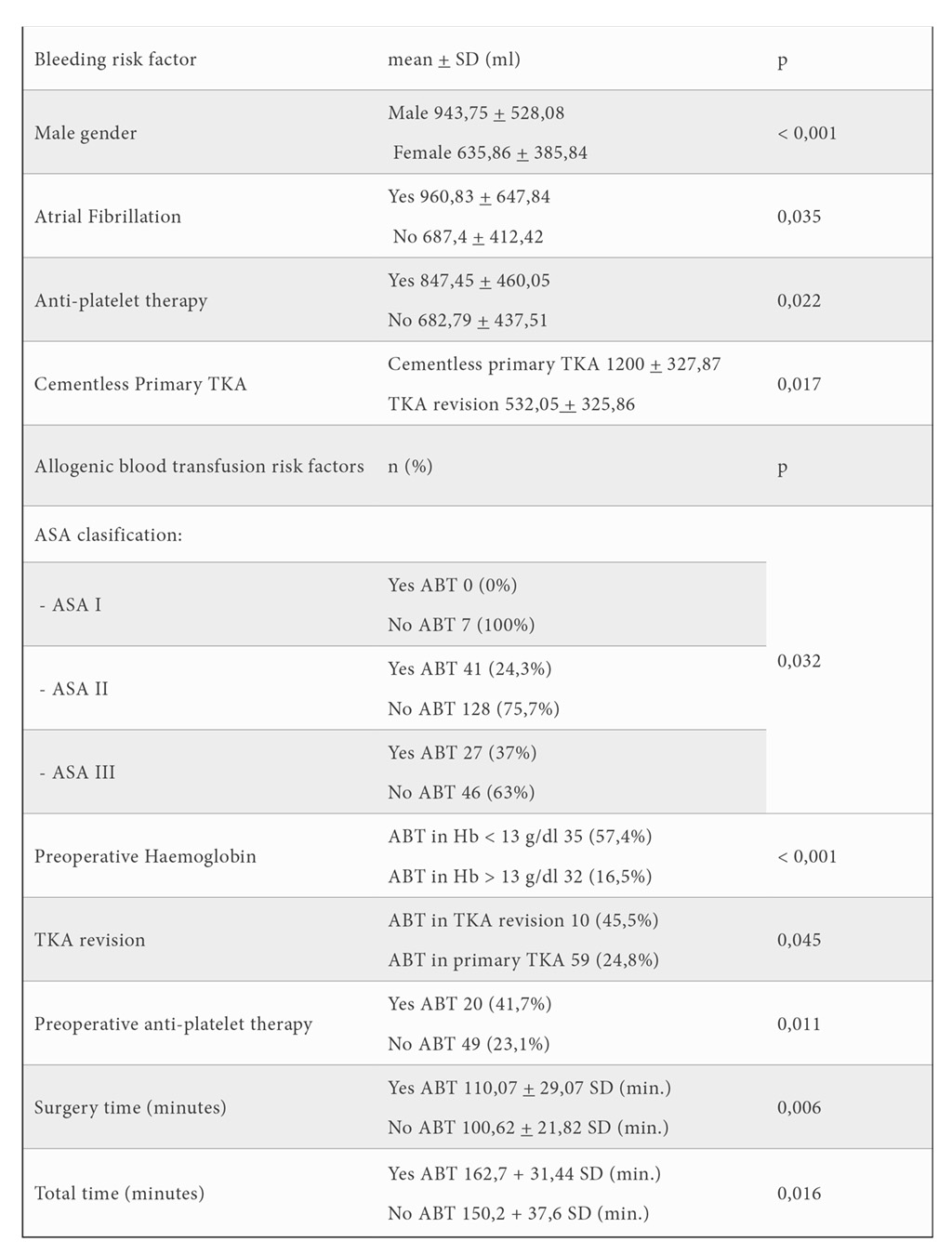
The ASA classification status > II (figure 4), preoperative Hb values < 13 g/dl, knee revision, APT, longer surgery time and total time were identified as risk factors for ABT (table 3). Moreover, a higher preoperative Hb level was associated with a lower risk of transfusion (RR=1.959 [1.455-2.639]).
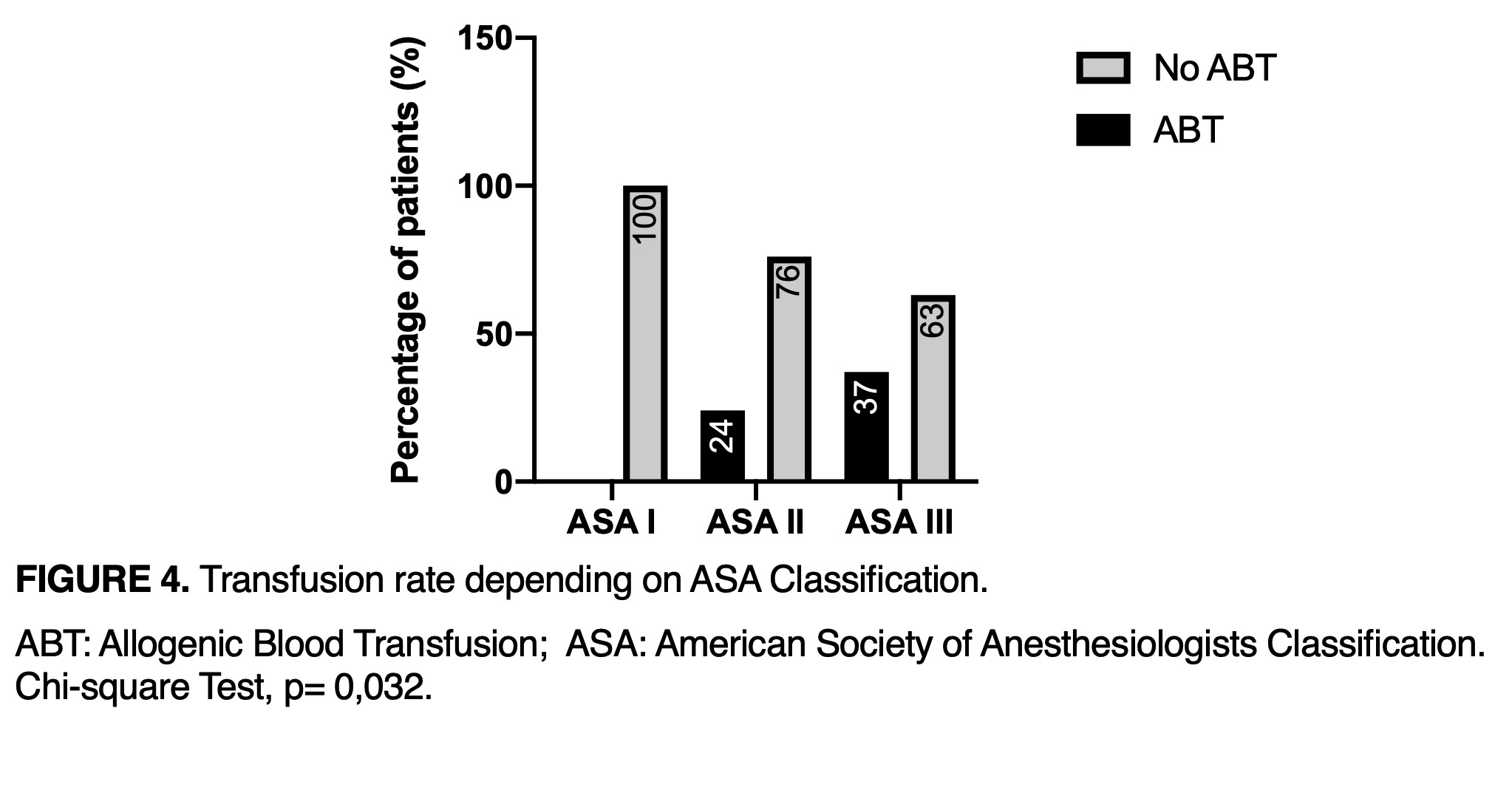
ABT: Allogenic blood transfusion; ASA: American Society of Anesthesiologists Classification.
Chi-square Test, p=0,032
Anesthesia or postoperative analgesia technics did not influence the rate of ABT. Patients receiving ABT presented lower hemoglobin and hematocrit values (p<0.001), and a longer PACU time (+7 hours in PACU, p<0.001) and medium LOS (+2.5 days in LOS p=0.026).
DISCUSSION
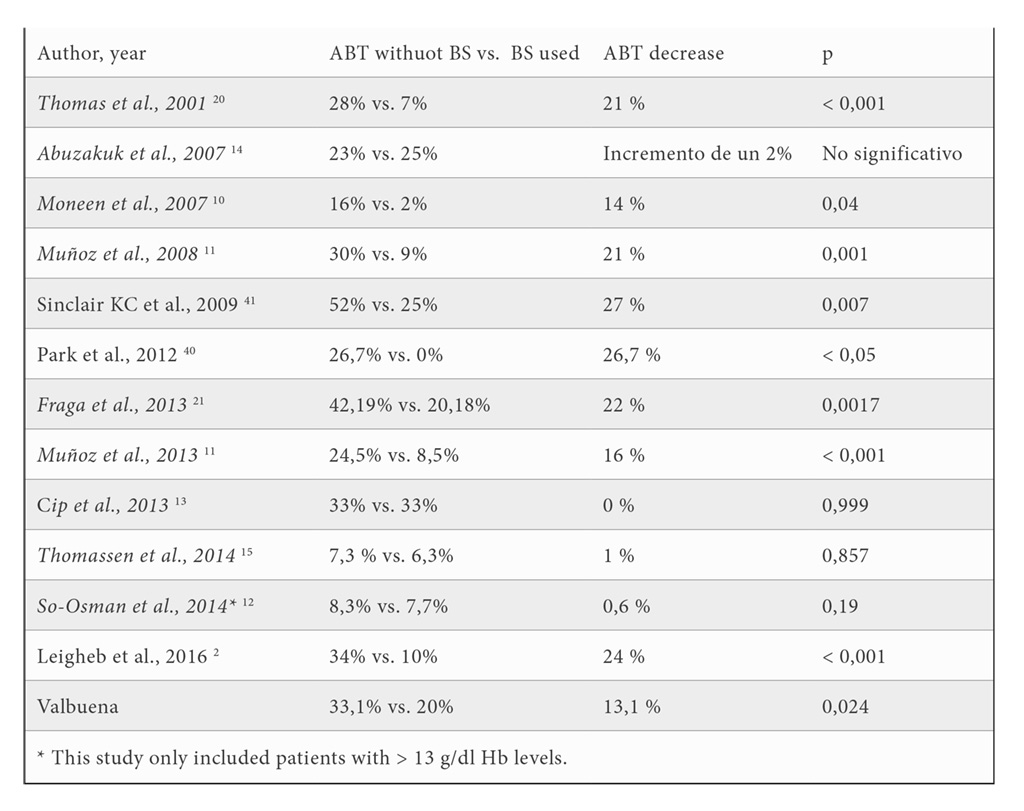
In this retrospective observational study, we observed that BS strategies are an effective tool to achieve a significant reduction in ABT, and this is consistent with most published studies (table 4). Muñoz et al. also found a reduction in the number of blood units transfused (11). We couldn’t confirm this reduction in our study because the sample size was not calculated for this variable. However, other authors like So-Osman el al. (12) did not either find any difference in transfusion rate, but their patients presented preoperative hemoglobin levels superior to 13 g/dl. No difference was found either by Martin y von Strempel, Abuzakuk et al. (13), Tomasen et al. (14) and Cip et al. (15) whose patients presented any rank of Hb. Nevertheless, Tomasen’s study was performed in patients who were optimized preoperatively with a restrictive transfusion program. They received pre- and postoperative EPO treatment. This explains the very low transfusion rate (7.1%) hiding the positive effect of BS on ABT (15).
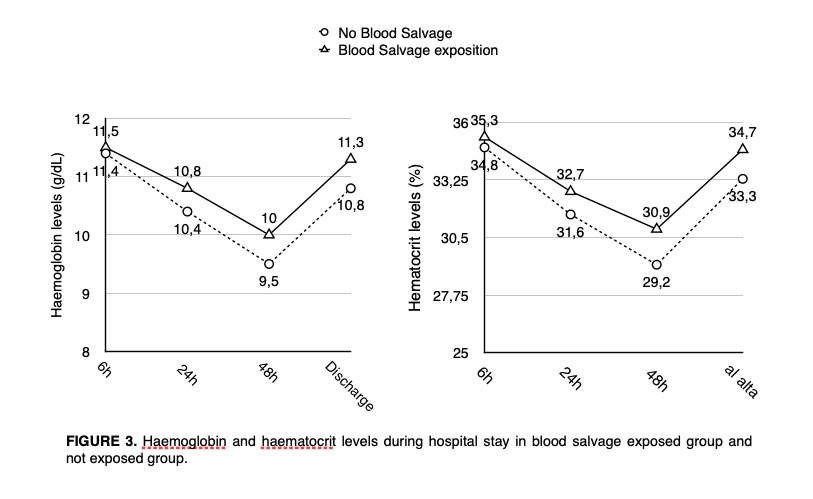
Patients with BS had higher Hemoglobin and Hematocrit values than those without BS during their whole hospital stay. They presented a decrease of Hb and Hematocrit at 48 hours and recovered on the fifth day. This trend is similar to the one described by Zhou et al.(16) and Mayer-Rollnik(17). Kourtzis et al. (12), Sinclair et al. (13), Kirkos et al. (18) y Biarnés et al. (19) also demonstrated the efficacy of BS in maintaining higher postoperative Hb and Htc values. Moonen et al. (10) and Tomasen et al. (15) described higher albeit non significative differences in the postoperative Hb values in the BS group. Our population’s clinical and demographic characteristics were similar to other studies about TKA and total knee replacement (10,12,13,19,20,21).
The transfusion rate in our study was lower than that of other series. Gombotz et al. showed (22) is a wide variability between 20 and 50% (23.9% presented preoperative anaemia, Hb < 13 g/dl) was similar to those of Saleh E. et al. (4) (19.96%), Hare et al. (23) (20%) and those estimated by WHO for the world (25%) and Europe (28.7%) (24,25). However, patients in the study of Saleh E. et al. (26) presented more severe anaemia than those in our study. This high prevalence of preoperative anaemia might be due to a higher incidence of rheumatoid arthritis in their cohort of patients. This inflammatory disease is often accompanied by anaemia and the risk of ABT is increased three-fold (27,28).
The progressively aging population increases the need for arthroplasty. Associated comorbidity, mainly cardiovascular pathology, increases the need for anti-platelet and anticoagulant therapy. Very few studies address the issue of the influence of APT and anticoagulant therapy on orthopaedic surgery bleeding. We identified APT and LMWHT as the most important risk factors for bleeding and ABT as in Burger et al. (29) studied this outcome in a meta-analysis, as well as did the authors of the POISE-2 clinical trial (Perioperative Ischemia Evaluation) (30,31). The latter did not support keeping preoperative APT in non-cardiac surgeries (32). Gombotz et al. (22) found also in TKR, THR and coronary by-pass, an increase in ABT with simple and double APT (43.8% and 62.6% respectively) at a similar rate to our results. Only found two retrospective studies described an increase in bleeding and/or ABT with no association with preoperative APT (33,34). Our study confirm these results.
We could not identify anticoagulation as a ABT risk factor despite other studies having shown it to be so (35). Likewise, ASA Classification status > 3 was identified as a risk factor for complications during TKA recovery like anaemia and ABT. Similarly, preoperative anaemia is one of the most important and most studied transfusion risk factors, patients with Hb < 11 g/dl being those who would benefit most from preoperative hemoglobin optimization and blood-saving techniques like postoperative blood salvage (9, 27).
Surgery time has been widely identified in the literature as another bleeding and ABT risk factor. Therefore, reducing surgery time as much as possible improves productivity and reduces bleeding and ABT (10, 36, 37, 38). Equally, it has also been shown that ABT increases LOS and PACU time significantly with much lower Hb during the stay (11, 22).
In view of these results, the use of postoperative BS in TKA remains a good technique to reduce the need for ABT, minimizing the associated morbidity and mortality on this kind of surgery. Changes of practice in the last years have permitted to enter in the era of tranexamic acid, which has demonstrated its effectiveness. Nevertheless, there is a lack of evidence about its safety and the incidence of severe adverse events in high risk patients. In most randomized clinical trials, patients with thromboembolic diseases were excluded (39, 40). Fillingham et al. published a meta-analysis in 2018 and didn’t either encounter any data concerning the incidence of arterial thrombosis (39). So, the published results on safety of tranexamic acid cannot be applied to patients with high risk of deep vein thrombosis and pulmonary embolism. However, high risk patients with an ASA > 3 classification status didn’t present a higher risk of developing vein thromboembolism in TKA, according to Fillingham meta-analysis (39).
CONCLUSIONS
In view of this results, we will be able to detect preoperatively those patients with a higher risk of hemorrhage and/or bleeding. This will allow us to improve their postoperative care after TKA. In the same way, all efforts must be focused on offering those patients with preoperative anaemia an effective optimization, which is one of the most important pillar of Patient Blood Management.
The use of blood salvage in TKA showed benefits reducing allogenic blood transfusion and length of hospital stay. Postoperative blood salvage would remain an effective, safe and cheap alternative to tranexamic acid, especially in those patients with a high risk of thromboembolism events operated of TKA, in which the use of tranexamic acid remains controversial.
BIBLIOGRAPHY
- Kuperman EF, Schweizer M, Joy P, Gu X, Fang MM. The effects of advanced age on primary total knee arthroplasty: a meta-analysis and systematic review. BMC geriatr. 2016; 16: 41.
- Leigheb M, Pogliacomi F, Bosetti M et al. Postoperative blood salvage versus allogeneic blood transfusion in total knee and hip arthroplasty: a literature review. Acta Biomed. 2016; 87 (Suppl 1): 6-14.
- García-Erce JA, Manuel S, Cuenca J, Ortega P. La hemoglobina preoperatoria como único factor predictor de las necesidades transfusionales en la artroplastia de rodilla. Rev Eso Anestesiol Reanim. 2002; 49; 254-260.
- Shander A, Van Aken H, Colomina MJ, et al. Patient blood management in Europe. Br J Anaesth. 2012; 109(1): 55-68.
- Smilowitz NR, Oberweis B, S.Nukala S et al. Association between anemia, bleeding, and transfusion with long-term mortality following noncardiac surgery. Am J Med. 2016; 129(3): 315-323. e2.
- Meier J, Filipescu D, Kozek-Langenecker S et al. Intraoperative transfusion practices in Europe. Br J Anaesth. 2016; 116(2): 255-261.
- Horstmann W, Slappendel R, Van Hellemond G, Castelein R, CPM. V. Safety of retransfusion of filtered shed blood in 1819 patients after total hip or knee arthroplasty. Transfus Altern Transfus Med. 2010; 11(2): 57-64.
- Gharehbaghian A, Haque KM, Truman C et al. Effect of autologous salvaged blood on postoperative natural killer cell precursor frequency. Lancet. 2004; 363(9414): 1025-1030.
- Kirkos JM, Krystallis CT, Konstantinidis PA, Papavasiliou KA, Kyrkos MJ, Ikonomidis LG. Postoperative re-perfusion of drained blood in patients undergoing total knee arthroplasty: is it effective and cost-efficient? Acta orthopaedica Belgica. 2006; 72(1): 18-23.
- Moonen AF, Thomassen BJ, van Os JJ, Verburg AD, Pilot P. Retransfusion of filtered shed blood in everyday orthopaedic practice. Transfusion Med. 2008; 18(6): 355-359.
- Muñoz, M, Ariza D, Campos A, Martín-Montañez E, Pavia, J. The cost of post-operative shed blood salvage after total knee arthroplasty: an analysis of 1,093 consecutive procedures. Blood Transfus. 2013;11(2): 260-271.
- So-Osman C, Nelissen RG, Koopman-van Gemert AW et al. Patient blood management in elective total hip- and knee-replacement surgery (part 2): a randomized controlled trial on blood salvage as transfusion alternative using a restrictive transfusion policy in patients with a preoperative haemoglobin above 13 g/dl. Anesthesiology. 2014; 120(4): 852-860.
- Cip J, Widemschek M, Benesch T, Waibel R, Martin A. Does single use of an autologous transfusion system in TKA reduce the need for allogenic blood?: a prospective randomized trial. Clin Orthop Relat Res. 2013; 471(4): 1319-1325.
- Abuzakuk T, Senthil Kumar V, Shenava Y et al. Autotransfusion drains in total knee replacement: Are they alternatives to homologous transfusion? Int Orthop, 2007; 31(2): 235-239.
- Thomassen, BJ, den Hollander PH, Kaptijn HH, Nelissen RG, Pilot P. Autologous wound drains have no effect on allogeneic blood transfusions in primary total hip and knee replacement: a three-arm randomised trial. Bone Joint J. 2014; 96-B(6): 765-771.
- Zhou Q, Zhou Y, Wu H et al. Changes of haemoglobin and hematocrit in elderly patients receiving lower joint arthroplasty without allogeneic blood transfusion. Chin Med J (Engl). 2015; 128(1): 75-78.
- Mayer-Rollnik S, Harms C, Bernasconi L et al. Evaluation of autologous retransfusion from a closed suction drainage system for patient blood management in elective total hip and knee replacement: a two cohort study. Eur J Anaesthesiol. 2020; 37(3): 180-186.
- Kourtzis N, Pafilas D, Kasimatis G. Blood saving protocol in elective total knee arthroplasty. Am J Surg. 2004; 187: 261-267.
- Crescibene A, Martire F, Gigliotti P, Rende A, Candela M. Postoperative autologous reinfusion in total knee replacement. J Blood Transfus. 2015; 2015: 826790.
- Thomas D, Wareham K, Cohen D, Hutchings H. Autologous blood transfusion in total knee replacement surgery. Br J Anaesth. 2001; 86(5): 669-673.
- Fraga G, Ramos-Luengo A, Miyagi M, Rodriguez-Tato P, Berberana M, Gonzalez L. Decrease in allogenic transfusions due to the spread of use of postoperative retransfusion systems in knee replacement surgery. Rev Esp Anestesiol Reanim. 2013; 60(6): 308-312.
- Gombotz H, Rehab PH, Shander A, Hofmann A. Blood use in elective surgery: the Austrian benchmark study. Transfusion. 2007; 47(8): 1468-1480.
- Hare GM, Tsui AK, Ozawa S, Shander A. Anaemia: can we define haemoglobin thresholds for impaired oxygen homeostasis and suggest new strategies for treatment? Best Pract Res Clin Anaesthesiol. 2013; 27(1): 85-98.
- Clevenger B, Richards T. Pre-operative anaemia. Anaesthesia. 2015; 70(Suppl 1): 20-28, e6-8.
- Auerbach M, Goodnough LT, Shander A. Iron: the new advances in therapy. Best Pract Res Clin Anaesthesiol. 2013; 27(1): 131-140.
- Saleh E, McClelland DB, Hay A, Semple D, Walsh TS. Prevalence of anaemia before major joint arthroplasty and the potential impact of preoperative investigation and correction on perioperative blood transfusions. Br J Anaesth. 2007; 99(6): 801-808.
- Sizer SC, Cherian JJ, Elmallah RD, Pierce TP, Beaver WB, Mont MA. Predicting blood loss in total knee and hip arthroplasty. Orthop Clin North Am. 2015; 46(4): 445-459.
- Prasad N, Padmanabhan V, Mullaji A. Blood loss in total knee arthroplasty: an analysis of risk factors. Int Orthop. 2007; 31(1): 39-44.
- Burger W1, Chemnitius JM, Kneissl GD, Rücker G. Low-dose aspirin for secondary cardiovascular prevention -cardiovascular risks after its perioperative withdrawal versus bleeding risks with its continuation – review and meta-analysis. J Intern Med. 2005; 257(5): 399-414.
- Ghadimi K, Thompson A. Update on perioperative care of the cardiac patient for noncardiac surgery. Curr Opin Anaesthesiol. 2015; 28(3): 342-348.
- Kristensen SD, Knuuti J, Saraste A et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur J Anaesthesiol. 2014; 31(10): 517-573.
- McCunniff PT, Young ES, Ahmadinia K, Kusin DJ, Ahn UM, Ahn NU. Chronic antiplatelet use associated with increased blood loss in lumbar spinal surgery despite adherence to protocols. Orthopedics. 2016; 39(4): e695-700.
- Schwab PE, Lavand’homme P, Yombi J, Thienpont E. Aspirin mono-therapy continuation does not result in more bleeding after knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2017; 25(8): 2586-2593.
- Meier R, Marthy R, Saely CH, Kuster MS, Giesinger K, Rickli H. Comparison of preoperative continuation and discontinuation of aspirin in patients undergoing total hip or knee arthroplasty. Eur J Orthop Surg Traumatol. 2016; 26(8): 921-928.
- Leitner L, Musser E, Kastner N et al. Impact of preoperative antithrombotic therapy on blood management after implantation of primary total knee arthroplasty. Sci Rep. 2016; 6: 30924.
- Hrnack SA, Skeen N, Xu T, Rosenstein AD. Correlation of body mass index and blood loss during total knee and total hip arthroplasty. Am J Orthop (Belle Mead NJ). 2012; 41(10): 467-471.
- Noticewala MS, Nyce JD, Wang W, Geller JA, Macaulay W. Predicting need for allogeneic transfusion after total knee arthroplasty. J Arthroplasty. 2012; 27(6): 961-967.
- Frisch NB, Wessell NM, Charters MA, Yu S, Jeffries JJ, Silverton CD. Predictors and complications of blood transfusion in total hip and knee arthroplasty. J Arthroplasty. 2014; 29(9 Suppl): 189-192.
- Fillingham YA, Ramkumar DB, Jevsevar DS et al. The safety of tranexamic acid in total joint arthroplasty: a direct meta-analysis. J Arthroplasty. 2018; 33(10): 3070-3082.e1.
- Park KH, Lee SR, Jin JM, Moon MS. The efficacy and safety of postoperative autologous transfusion of filtered shed blood and anticoagulant prophylaxis in total knee arthroplasty patients. Knee Surg Relat Res. 2012; 24(1): 14-18.
- Sinclair KC, Clarke HD, Noble BN. Blood Management in Total Knee Arthroplasty: A Comparison of Techniques. Orthopedics. 2009 Jun;32:19.
CONFLICT OF INTEREST STATEMENT
The authors of this article declare that they have no conflict of interest with respect to what is expressed in this work.
Isabel Valbuena
Department of Anesthesiology and Intensive Care Medicine. HU La Paz.
Paseo De La Castellana 261 · 28046 Madrid, Spain.
Tlf.: +34 91 159 47 34 | E-Mail: isa_valbuena_gomez@hotmail.com
Año 2022 · número 139 (01) · páginas 67 a 77
Enviado: 03.04.22
Revisado: 06.04.22
Aceptado: 14.04.22