

Abstract
Introduction: Nowadays, practical learning is an important part of Medicine degree, and even more in low- and middle-income countries (LMICs). To teach some regular techniques, such as peripheral vein catheterization (PVC), simulation models are being used. They create safer realistic scenarios for students to practice and feeling safer. There are several different techniques and models for teaching this performance, to learn several techniques. The aim of this study is to validate a new placenta simulation model for peripheral vein canalization learning.
Methods: We designed an observational study on ten sixth-grade medicine students who performed ten procedures in placentas plus ten other procedures in mannequins, the gold standard simulation model. During the catheterization technique or activity, successful and failed punctures with each model were registered and this data was used to elaborate learning curves with the Cummulative sum (CUSUM) method.
Results: Placental model proved to be as useful as mannequins for learning the technique. Most of the students acquired the competence in PVC, with a rate of success of at least an 80%, after ten procedures. Also, satisfaction surveys were handed over for students to evaluate their learning process. Most of them expressed to have learnt better with placental model and found simulation use very positive for medical students training.
Discussion: The new placenta model was at least as good as the standard. 10 attempts of PVC were enough to learn the skill in most students with any of both models. Placenta availability is cheap and can be used wherever deliveries may take place.Resumen
Introducción: Hoy en día, el aprendizaje práctico es una parte importante de los estudios para el Grado de Medicina, y más aún en los países de ingresos bajos y medios (LMICs). Para enseñar algunas técnicas habituales, como el cateterismo de venas periféricas (PVC), se utilizan modelos de simulación. Crean escenarios realistas más seguros para que los estudiantes practiquen, sintiéndose más seguros. Existen varias técnicas y modelos diferentes para enseñar esta actuación y aprender esta y otras técnicas. El objetivo de este estudio es validar un nuevo modelo de simulación de placenta para el aprendizaje de la canalización de venas periféricas.
Métodos: Diseñamos un estudio observacional en diez estudiantes de sexto grado. estudiantes de medicina que realizaron diez procedimientos en placentas más otros diez procedimientos en maniquíes, con el modelo de simulación estándar. Durante la técnica de cateterismo, se registraron punciones exitosas y fallidas con cada modelo y estos datos se utilizaron para elaborar curvas de aprendizaje con el método CUSUM (suma acumulativa de casos).
Resultados: El modelo placentario demostró ser tan útil como los maniquíes para el aprendizaje de la técnica. La mayoría de los estudiantes adquirieron la competencia en PVC, con una tasa de éxito de al menos un 80%, tras diez procedimientos. para que así los estudiantes evalúen su proceso de aprendizaje. La mayoría de ellos expresaron haber aprendido mejor con el modelo placentario y encontraron el uso de la simulación muy positivo para la formación de los estudiantes de medicina.
Discusión: El nuevo modelo de placenta era al menos tan bueno como el estándar. 10 intentos de PVC fueron suficientes para aprender la habilidad en la mayoría de los estudiantes con cualquiera de ambos modelos. La disponibilidad de placenta es económica y se puede utilizar dondequiera que se realicen partos.Keywords: Teaching; Medical students; Peripheral vein catheterization; Placenta; CUSUM curves.
Palabras clave: Docencia; Estudiantes medicos; Cateterización venosa periférica; Placenta; Curvas CUSUM.
Introduction
Practical skills acquisition is an important aspect of medical education in high income countries (HICs) and in LMICs. Medical students, nurses and non-physician anesthesia providers (NPAPs), must learn some basic competences. Among these skills, we can find peripheral vein canulation (PVC).
PVC is usually taught to medical students and other learners using simulation on plastic mannequins, that may be similar, or not, to real patients. Frequently mannequins may have been used by too many students, so it may be difficult to learn this skill. The problems with this conventional model are, the cost of the mannequins, the repeated use of them, the number of punctures at the same place and lack of realism of the model.
Mannequins are expensive, and are not available in many countries, or at peripheral hospitals or centers.
Placenta as a simulation model has been described for neurosurgical and vascular techniques (1) We have recently described and published a new model to teach medical students peripheral vein canalization using fresh human placenta. (2) The placenta model is a “closed blood circuit” full of veins in the fetal side of it, that are available to be used by tutorized medical students.
Training in practical skills can follow different methods. From the classic model that is the “see-one, do-one, teach-one” (3) to nowadays, the learning models have changed significatively. Learning must be based on the competences and acquisition of skills (4). Each student, or resident, requires individual attention, which is not necessarily the same in all cases. The use of objective evaluation tools facilitates this individualization, while allowing planning the average number of procedures necessary to acquire the selected competence that is going to be evaluated. To analyze the acquisition of competencies, while learning different techniques in some particular fields, such as anesthesia (5) and surgery, the Cumulative Sum (CUSUM) statistical method is frequently used (6). CUSUM method allows the development of learning curves that reflect how the performance of the technique improves over time, after successive attempts.
The proposed hypothesis is that the placenta is as reliable as the conventional method with mannequins, or even more reliable than the simulation mannequin for learning PVC.
Our goal is to validate the simulation model with placenta, compared with the use of mannequins, for learning PVC in a group of sixth-year medical school students.
METHODS
After Local Hospital and University Research Ethics Committee/Institutional Review Board approval (PI-4991. Madrid, November 29th 2021. President Ethics Committee Dr. Emma Fernandez-Uzquiano) and written informed consent obtained of all women and students, we designed a unicentric observational study based on a teaching activity called “peripheral vein cannulation” (PVC) included in the official program of our medical school in conventional simulation mannequins and in human fresh placenta after delivery. We used 20G standard iv cannulas.
We studied the performance on this skill, PVC, of 10 volunteer students at 6th year medical school. We divide the students in 2 groups of 5 persons each. Group 1 started the PVC at the hospital obstetric delivery suite with human placenta specimens obtained from recently delivered women. Group 2 started the PVC with conventional mannequins in the simulation department (room) of our medical school. Once persons in every group had performed 10 attempts of PVC in their initially assigned model, they exchanged to the other one and they performed 10 additional attempts of PVC.
The placentas were selected according to the following criteria: Informed consent of the mother and the student, regular size of the specimen (excluded small specimens and coagulated placental vessels), integrity of the placental tissue and its venous net and a working cord clamp closing the cord, to avoid placental exsanguination. An exclusion criterion was if the placenta had to be sent to the pathology department for any reason.
The total number of attempts was 200 (10 procedures each student on each model). (Fig. 1)

For anonymization of the students and the correct handling of the information, each participant student received an identification code with 3 values: first the student itself with a number from 1 to 10, second “a” for placenta group or “b” for mannequin group, third which number of performed procedure, also from 1 to 10. So, the record 1 a 10 means; student number 1, uses placenta (a) for his/her 10th attempt.
We considered “SUCCESS” of the PVC, when it was introduced the iv cannula in the selected vein and blood or fluid in the mannequin model flowing through this catheter on the first attempt. “FAILURE” was considered if any of the previous criteria was not fulfilled.
We collected all data in an anonymized database Microsoft® Excel® 2019 MSO (version 2202 compilation 16.0.14931.20128).
To compare the data collected, the absolute frequency and percentage of the qualitative variables are provided and, of the quantitative ones, the mean and standard deviation, if they follow a parametric distribution, or the median and range (non-parametric distribution). For the hypothesis contrast of the qualitative variables, the results were grouped into contingency tables and the Pearson Chi Square statistical test was applied. For quantitative variables, the Mann-Whitney-Wilcoxon test (non-parametric test) was applied.
The CUSUM statistical method (6) was applied, and a learning curve was developed for each student. If a curve reaches or crosses the lower limit, with a value on the Y axis of -2.24, it means that the success rate has been equal to or greater than 80% and the objective of acquiring the skill has been reached. If the curve exceeds the upper limit, with a value on the Y axis of 2.24, it means that the student has had a success rate of less than 60%, which is considered unacceptable for the acquisition of the competence and indicates that learning is uncontrolled. The space between both limits corresponds to a success rate of 60-80% and indicates that learning is under control.
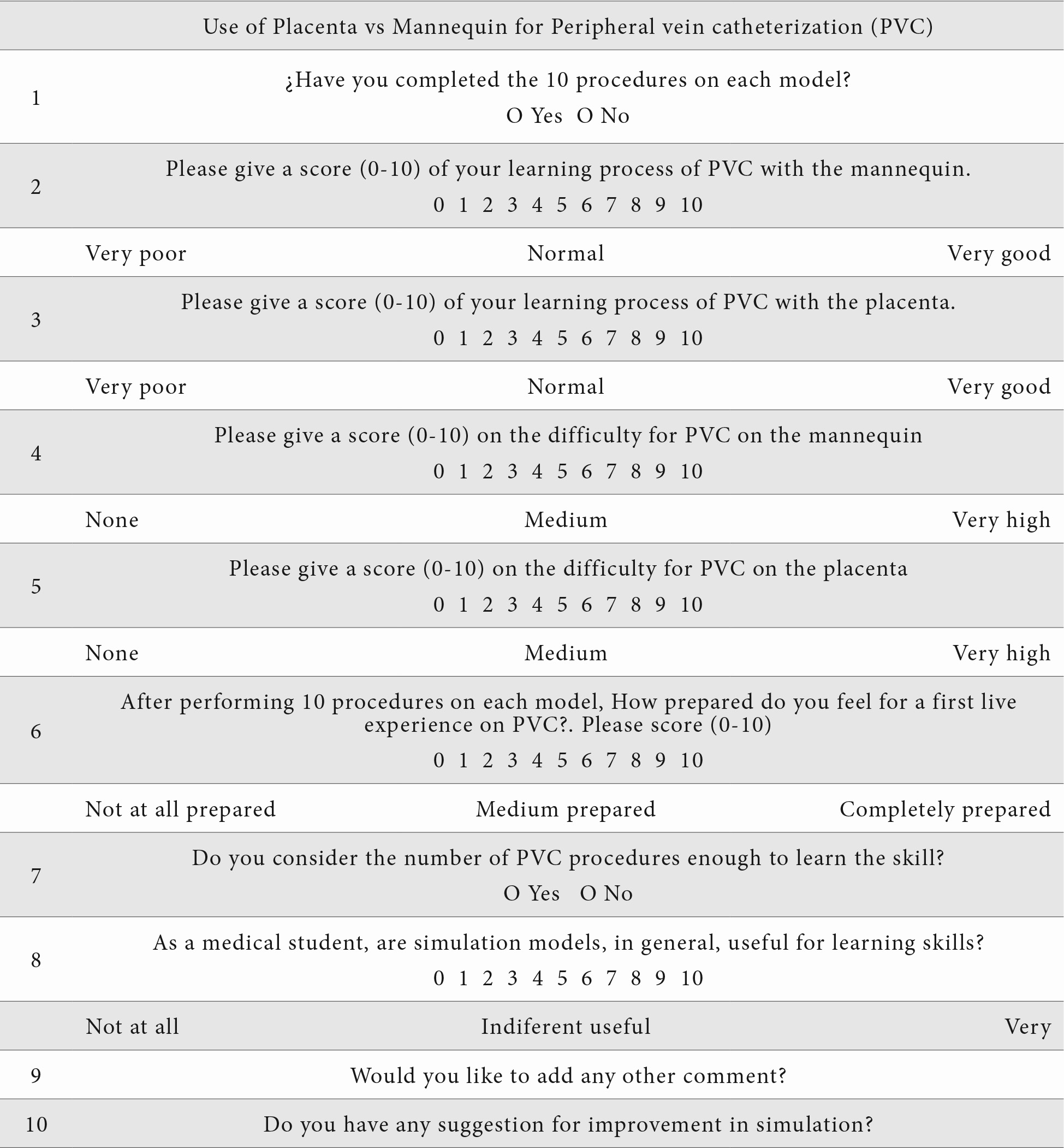
After completion of this part of the study, the participants were given an anonymous questionnaire to assess their attitude towards PVC, after having tried both learning models. Questions 1 and 7 are dichotomous, with yes or no answers, questions 2-6 and 8 admit answers from 0 to 10, within a Likert scale (7), and questions 9 and 10 are open questions. (Table 1)
Results
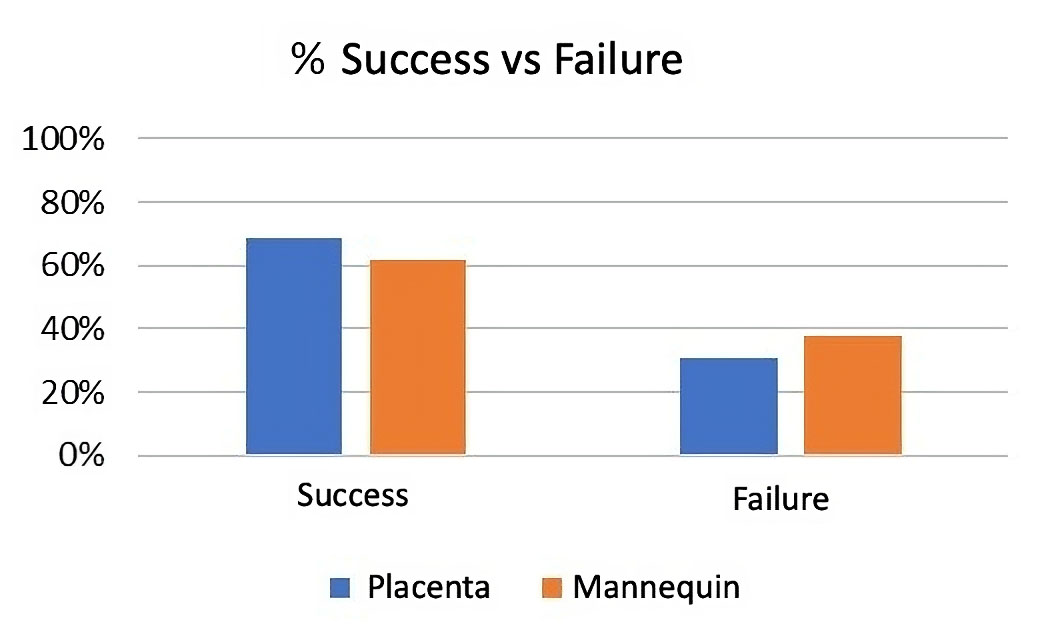
100% of students performed the procedures both in placenta and mannequin. Data collection and procedures took 3 weeks, from January 20th, 2022 to February 8th 2022. The global percentage of success and failures on each group is shown in (Fig.2). No differences were found between groups (Pearson Chi square p=0,3).
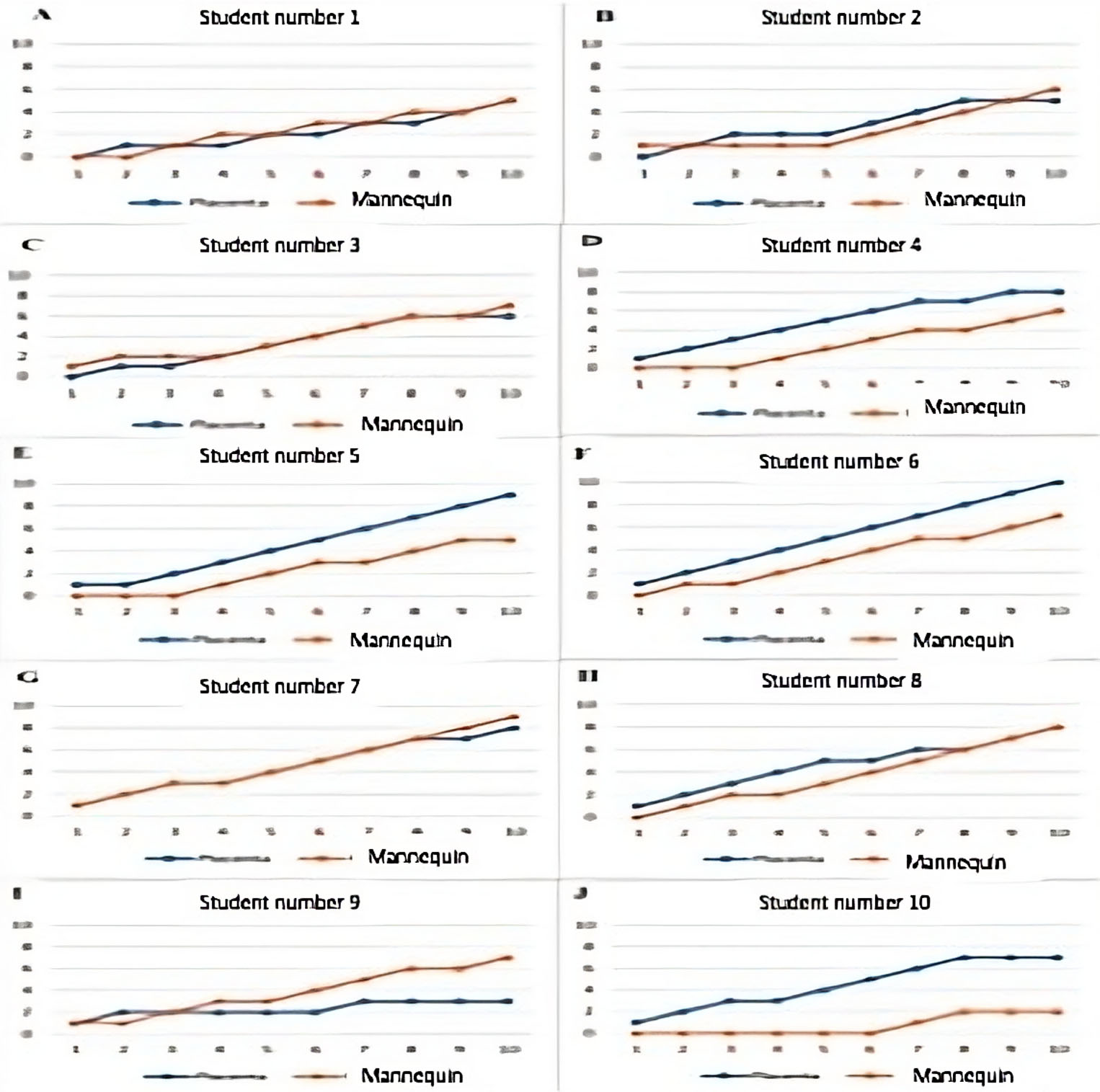
We compared each student success rate with each model, applying Chi square test. 8 of these students did not show differences in success rate (p>0,05), and student 5 and 10 showed differences (p=0,05 and p=0,02 respectively) (Fig.3)
We tried to determine if 10 attempts per student were enough to reach the competence. For that goal, we used CUSUM method to build learning curves.
In group “1” (placenta), all the students, except numbers 1 and 9, reached the competence after a mean of 5 attempts (range 4-8). In group “2” (mannequins) all the students, except numbers 1 and 10, reached the competence after a mean of 6 attempts (range 5-9). Neither of the students were under the unacceptable level of competence. (Fig.4)
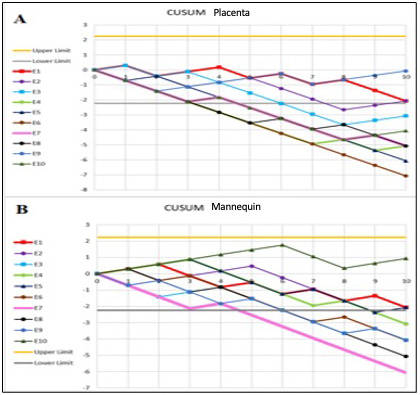
channels (0-10). Y axis: CUSUM value. E1: student 1; E2: student 2; E3: student 3; E4: student 4; E5: student 5; E6: student 6; E7: student 7; E8: student 8; E9: student 9; E10: student 10. In graph A, all the curves cross the lower limit after 5 (range 4-8) trials, except E1 and E9. In graph B, all the curves cross the lower limit after 6 (range 5-9) trials, except E1 and E10.
We compared, using Mann Whitney-Wilcoxon test, the number of required attempts required for each student to reach the competence. We could not find differences (p=0,09). There is a trend that favors the placenta group.
Finally, we analyzed the subjective evaluation survey given to the students, with scores from 0 to 10. The learning experience of the PVC technique with mannequins received a score equal to or greater than 7 in six students, obtaining the highest score (9-10) in three students. Learning PVC with the placental model obtained a rating higher than 7 in 100% of the students and the highest rating of 10, was given by eight students. The mean difficulty subjectively recorded by the students, when performing PVC in a mannequin was 6.8 and in the placenta was 3,9. Most of the students, after the study, considered themselves prepared for PVC in vivo with a mean score of 7,4. The usefulness of the simulation models for learning the PVC technique received an average score of 9,2.
Discussion
The placental model has proven to be at least as useful for learning PVC as mannequins, considered as a current reference model in 6th year medical students. Furthermore, the number of attempts required to reach channeling proficiency was similar comparing both models.
Numerous simulation studies use mannequins for learning venous cannulation in nursing (8) and medical (9) students. There are also publications on the use of cadavers (10) and other simpler venipuncture devices (11). This is the first description that an attempt has been investigated to validate a human placenta model for learning this technique, as suggested by our group recently (2). The fact that the activity under study (PVC), can be performed and quantified in the placenta, determines its content validity as a simulation model. In addition, the similarity of results in the placenta and the reference model (mannequin) determines their concurrency validity, as it is compared to “gold standard”. These concepts were defined by McDougall in 2007 (12) on validation criteria for surgical simulators and have served as a reference for other authors (13).
It is not only interesting to know that the placenta model contributes to learning, but also to what extent it may serve as a preparation for students to face the live PVC in their future patients. The usefulness of the CUSUM curves is based on setting the level of learning from which it is considered that the student masters the technique sufficiently to reproduce it safely in the current clinical practice. The use of these curves in Medicine is common to assess the progress of residents and students acquiring a skill in procedures of some technical difficulty, such as orotracheal intubation (14) or epidural anesthesia (5, 15), among other skills.
There are publications of studies similar to the present one, in which the puncture was tested in patients (16) or in mannequins (8), and with ten cannulations success rates of 67-77% were achieved. In our study, ten punctures were enough for at least eight students in each of the models tested to master the technique. This fact, raises the need to individualize the number of punctures in students who require more attempts, since the percentage of successes set to acquire the competence (80%) could be very strict. This conclusion is reached by other studies that have used the CUSUM method to assess the learning of medical residents (14, 15, 17).
Simulation is essential nowadays in our educational system, to teach the basics of clinical procedures and skills in the development of a safe environment for students. These fictional activities provide strategies to face real situations with greater skill, confidence, and adaptability (8, 18). The benefits for the student depend to a large extent on how they felt during their training (19). For this reason, it is important to consider the perception of the learning esperience of the students themselves, reflected in satisfaction surveys (16). In our study, all the participants considered in the surveys that they had learned the PVC technique with placentas very well and the students found PVC less difficult compared to the mannequins. In summary, the majority considered themselves ready to perform a PVC in vivo and highly evaluated the use of simulation for practical teaching in Medicine. We found several limitations to our study:
The availability and useful life of the mannequins is limited, favoring demotivation in the simulation session, since many of them are repeatedly punctured in the same places. Sometimes the filling mechanisms are technically complex and may require specific technical assistance.
The availability of placentas depends on whether there are deliveries at the hospital, although the fact that it is a biological product makes the variation in the arrangement of the placental veins similar to the variability also found in the daily clinical practice.
Simulation in LMICs is not an easy task, and different strategies have been developed to increase the access to this kind of resources.(20)
Low cost models have been implemented successfully in some LMICs (21)
Training programs, as SAFE programs developed by WFSA (22) and others (23) are useful, and in this context, our model is an additional strategy to teach the PVC skill easily and cheap.
The placenta model is cheaper, as it is a biological product that is usually discarded is reused, compared to a mannequin and its maintenance. Placental vessels look more real and versatile in the touch of the tissue and the thickness of the vessels, presenting different degrees of difficulty depending on the caliber of the vascular tree.
The PVC simulation activity with the placenta could be part of the students’ curriculum during their clinical rotation, under the direct supervision of the students’ teachers and/or tutors.
Financing statement
Support came solely from institutional and/or departmental sources.
CONFLICT OF INTEREST STATEMENT
The authors of this article declare that they have no conflict of interest with respect to what is expressed in this work.
BIBLIOGRAPHY
- ↑Oliveira MM, Wendling L, Malheiros JA et al. Human placenta simulator for intracranial-intracranial bypass: Vascular anatomy and 5 bypass techniques. World Neurosurg. 2018; 119: e694-e702.
- ↑Guasch E, Brogly N, Gilsanz F. Placental veins catheterization: a realistic simulation model for medical students. Anesthesiology. 2021; 135: 191-192.
- ↑Kotsis SV, Chung KC. Application of see one, do one, teach one concept in surgical training. Plast Reconstr Surg. 2013; 131: 1194-201.
- ↑Shorten G, Bahrey L, Bardia A et al. A consensus statement on the meaning, value and utility of training programme outcomes, with specific reference to anaesthesiology: a consensus statement on training programme outcomes. Eur J Anaesthesiol. 2023; 40: 596-607.
- ↑Guasch E, Diez J, Gilsanz F. Metodología CUSUM en la curva de aprendizaje de la punción epidural obstétrica en un hospital universitario. Rev Esp Anestesiol Reanim. 2010; 57: 11-15.
- ↑Aguirre Ospina OD, Ríos Medina AM, Calderón Marulanda M, Gómez Buitrago LM. Cumulative Sum learning curves (CUSUM) in basic anaesthesia procedures. Rev Colomb Anestesiol. 2014; 42: 142-153.
- ↑Cachia M, Balzan G, Pace-Bardon M et al. Simulation training for foundation doctors on the management of the acutely ill patient. Adv Med Educ Prac. 2015; 6: 657-663.
- ↑Ravik M, Havnes A, Bjork IT. Defining and comparing actions in two simulation modalities: Students training on a latex arm and each other´s arm. J Clin Nurs. 2017; 26: 4255-4266.
- ↑Chao A, Lai CH, Chan KC, Yeh CC, Yeh HM, Fan SZ, Sun WZ. Performance of central venous cathterization by medical students: a retrospective study of students´ logbooks. BMC Med Educ. 2014; 14:168.
- ↑Reid JDS, Vestrup JA. Use of a simulation to teach central venous access. J Med Educ. 1988; 63:196-197.
- ↑Torossian K, Benayoun S, Ottenio M, Brulez AC. Guidelines for designing a realistic peripheral venous catheter insertion simulator: a literature review. J Med Eng. 2019; 233: 963-978.
- ↑McDougall EM. Validation of surgical simulators. J Endourol. 2007; 21:244-247.
- ↑Musbahi O, Aydin A, Al Omran Y, Skilbeck CJ, Ahmed K. Current status of simulation in otolaryngology: a systematic review. J Surg Educ. 2017; 74: 203-215.
- ↑Rujirojindakul P, McNeil E, Rueangchira-urai R, Siripunt N. Learning curves of macintosh laryngoscope in nurse anesthetist trainees using cumulative sum method. Anesthesiol Res Pract. 2014; 2014: 850731.
- ↑Rodrigues de Oliveira Filho G. The construction of learning curves for basic skills in anesthetic procedures: an application for the cumulative sum method. Anesth Analg. 2002; 95: 411-416.
- ↑Jacobson AF, Winslow EH. Variables influencing intravenous catheter insertion difficulty and failure: an analysis of 339 intravenous catheter insertions. Heart Lung 2005; 34: 345-359.
- ↑Kollmann-Camaiora A, Brogly N, Alsina E, Gilsanz F. Use of the cumulative sum method (CUSUM) to assess the learning curves of ultrasound-guided continuous femoral nerve block. Rev Esp Anestesiol Reanim. 2017; 64: 453-459.
- ↑Jorgensen R, Laursen CB, Konge L, Pietersen PI. Education in the placement of ultrasound-guided peripheral venous catheters: a systematic review. Scand J Trauma Resusc Emerg Med. 2021; 29: 83.
- ↑Rodríguez González AM, Martínez Cervantes EA, Garza Garza GG, Rivera Cavazos A. Satisfacción en simulación en estudiantes de medicina. Educ Med Super. 2021; 35: e2331.
- ↑Malhotra K, Ali A, Soran V et al. Levelling the learning ground for healthcare professionals across the world through SIMBA: a mixed-methods study. BMJ Open. 2023; 13(7): e069109.
- ↑Irfanullah EA, Chandra A, Solaiman RH et al. Simulation training in a lower middle-income country: Supporting a new center and developing low-cost models for critical skill acquisition. Cureus. 2023;15(6): e40950. doi: 10.7759/cureus.40950.
- ↑https://wfsahq.org/es/our-work/education-training/safe-training/). Last accesed. January 2024.
- ↑Chou WK, Ullah N, Arjomandi Rad A et al. Simulation training for obstetric emergencies in low- and lower-middle income countries: a systematic review. Eur J Obstet Gynecol Reprod Biol. 2022; 276: 74-81.
Emilia Guasch
Hospital Universitario Fundación Jiménez Díaz
Av. de los Reyes Católicos, 2 · 28040 Madrid
Tlf.: +34 696 423 466 | E-Mail: emiguasch@hotmail.com
Año 2024 · número 141 (03) · páginas 201 a 208
Enviado: 08.05.24
Revisado: 12.05.24
Aceptado: 20.05.24